Department of General Practice, Amsterdam UMC, University of Amsterdam, Academic Medical Center, Amsterdam 1105 AZ, The Netherlands.
Amsterdam Public Health, Personalized Medicine, Amsterdam, The Netherlands.
Fam Pract. 2024 Oct 8;41(5):832-840. doi: 10.1093/fampra/cmae028.
Telephone triage is pivotal for evaluating the urgency of patient care, and in the Netherlands, the Netherlands Triage Standard (NTS) demonstrates moderate discrimination for chest pain. To address this, the Safety First Prediction Rule (SFPR) was developed to improve the safety of ruling out acute coronary syndrome (ACS) during telephone triage.
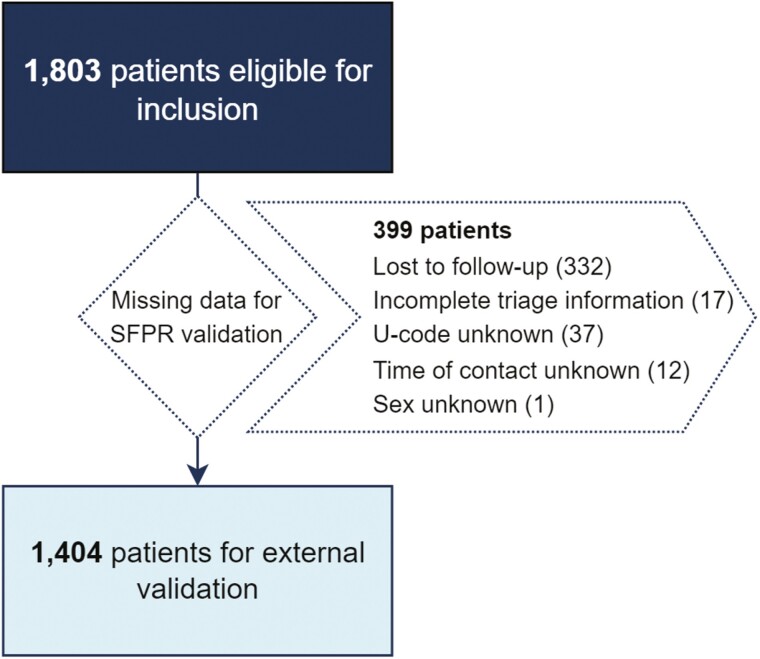
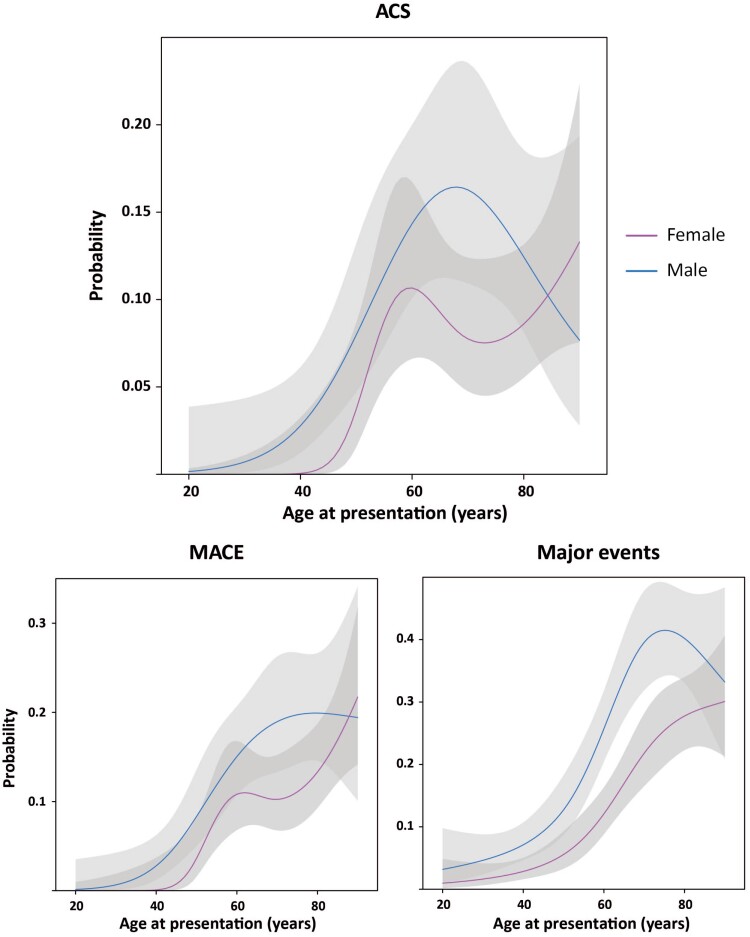
We conducted an external validation of the SFPR using data from the TRACE study, a retrospective cohort study in out-of-hours primary care. We evaluated the diagnostic accuracy assessment for ACS, major adverse cardiovascular events (MACE), and major events within 6 weeks. Moreover, we compared its performance with that of the NTS algorithm.
Among 1404 included patients (57.3% female, 6.8% ACS, 8.6% MACE), the SFPR demonstrated good discrimination for ACS (C-statistic: 0.79; 95%-CI: 0.75-0.83) and MACE (C-statistic: 0.79; 95%-CI: 0.0.76-0.82). Calibration was satisfactory, with overestimation observed in high-risk patients for ACS. The SFPR (risk threshold 2.5%) trended toward higher sensitivity (95.8% vs. 86.3%) and negative predictive value (99.3% vs. 97.6%) with a lower negative likelihood ratio (0.10 vs. 0.34) than the NTS algorithm.
The SFPR proved robust for risk stratification in patients with acute chest pain seeking out-of-hours primary care in the Netherlands. Further prospective validation and implementation are warranted to refine and establish the rule's clinical utility.
电话分诊对于评估患者护理的紧急程度至关重要,在荷兰,荷兰分诊标准(NTS)对胸痛具有中等程度的鉴别能力。为了解决这个问题,开发了安全第一预测规则(SFPR),以提高在电话分诊中排除急性冠状动脉综合征(ACS)的安全性。
我们使用 TRACE 研究的数据对 SFPR 进行了外部验证,TRACE 研究是一项在非工作时间的初级保健中进行的回顾性队列研究。我们评估了 ACS、主要不良心血管事件(MACE)和 6 周内主要事件的诊断准确性评估。此外,我们还比较了它与 NTS 算法的性能。
在纳入的 1404 名患者中(57.3%为女性,6.8%为 ACS,8.6%为 MACE),SFPR 对 ACS(C 统计量:0.79;95%-CI:0.75-0.83)和 MACE(C 统计量:0.79;95%-CI:0.76-0.82)具有良好的鉴别能力。校准结果令人满意,ACS 高危患者存在高估现象。SFPR(风险阈值 2.5%)的敏感性(95.8% vs. 86.3%)和阴性预测值(99.3% vs. 97.6%)较高,阴性似然比(0.10 vs. 0.34)较低,优于 NTS 算法。
SFPR 在荷兰寻求非工作时间初级保健的急性胸痛患者中证明了其风险分层的稳健性。需要进一步的前瞻性验证和实施,以完善和确定该规则的临床实用性。