Amsterdam UMC, University of Amsterdam, Academic Medical Center, Department of General Practice, Amsterdam Cardiovascular Sciences Research Institute, Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands.
Huisartsenorganisatie Noord-Kennemerland, Hertog Aalbrechtweg 5A, 1823 DL Alkmaar, The Netherlands.
Fam Pract. 2023 Feb 9;40(1):23-29. doi: 10.1093/fampra/cmac077.
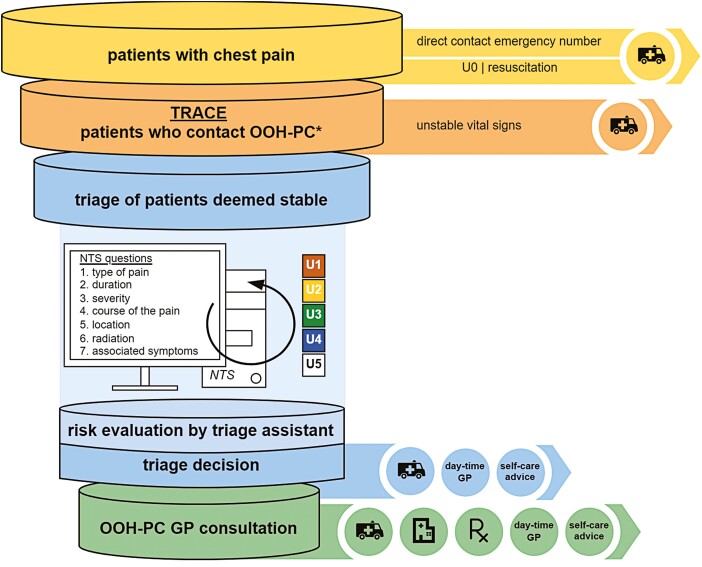
Telephone triage is fully integrated in Dutch out-of-hours primary care (OOH-PC). Patients presenting with chest pain are initially assessed according to a standardized protocol ("Netherlands Triage Standard" [NTS]). Nevertheless, little is known about its (diagnostic) performance, nor on the impact of subsequent clinical judgements made by triage assistants and general practitioners (GPs).
To evaluate the performance of the current NTS chest pain protocol.
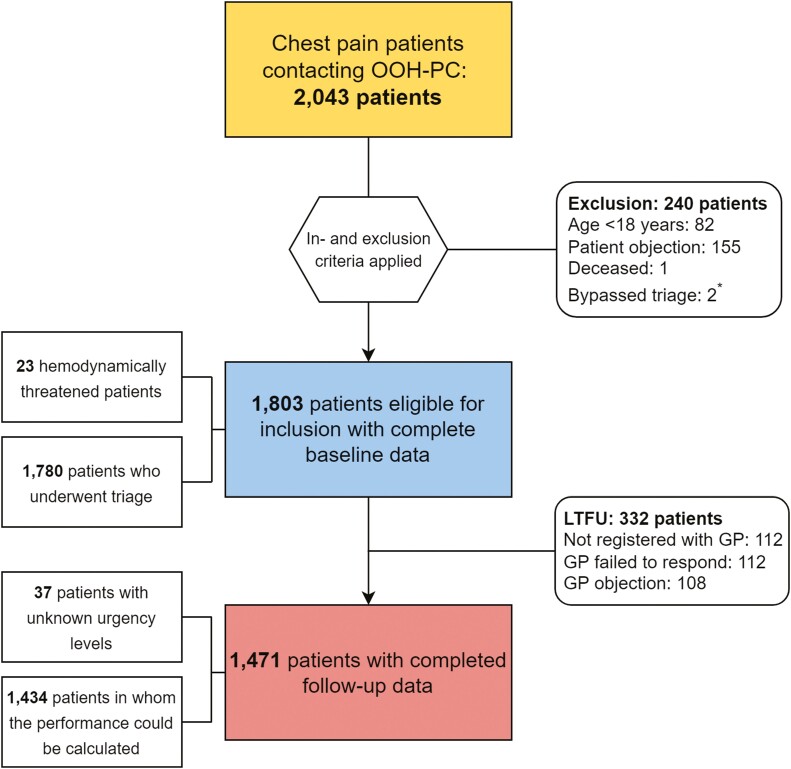
Observational, retrospective cohort study of adult patients with chest pain who contacted a regional OOH-PC facility in the Netherlands, in 2017. The clinical outcome measure involved the occurrence of a "major event," which is a composite of all-cause mortality and urgent cardiovascular and noncardiovascular conditions, occurring ≤6 weeks of initial contact. We assessed the performance using diagnostic and discriminatory properties.
In total, 1,803 patients were included, median age was 54.0 and 57.5% were female. Major events occurred in 16.2% of patients with complete follow-up, including 99 (6.7%) cases of acute coronary syndrome and 22 (1.5%) fatal events. NTS urgency assessment showed moderate discriminatory abilities for predicting major events (c-statistic 0.66). Overall, NTS performance showed a sensitivity and specificity of 83.0% and 42.4% with a 17.0% underestimated major event rate. Triage assistants' revisions hardly improved urgency allocation. Further consideration of the clinical course following OOH-PC contact did generate a more pronounced improvement with a sensitivity of 89.4% and specificity of 61.9%.
Performance of telephone triage of chest pain appears moderate at best, with acceptable safety yet limited efficiency, even after including further work-up by GPs.
电话分诊已完全融入荷兰非工作时间初级保健(OOH-PC)。出现胸痛的患者首先根据标准化协议(“荷兰分诊标准”[NTS])进行评估。然而,对于其(诊断)性能以及分诊助理和全科医生(GP)随后进行的临床判断的影响,我们知之甚少。
评估当前 NTS 胸痛协议的性能。
这是一项观察性、回顾性队列研究,纳入了 2017 年在荷兰一个地区性 OOH-PC 机构就诊的成年胸痛患者。临床结局测量包括“主要事件”的发生,主要事件是全因死亡率和紧急心血管和非心血管疾病的综合指标,发生在初始接触后≤6 周内。我们使用诊断和区分性能来评估性能。
共纳入 1803 例患者,中位年龄为 54.0 岁,57.5%为女性。在完成随访的患者中,有 16.2%发生了主要事件,其中包括 99 例(6.7%)急性冠状动脉综合征和 22 例(1.5%)致命事件。NTS 紧急程度评估对预测主要事件具有中等的区分能力(C 统计量为 0.66)。总体而言,NTS 的性能表现为 83.0%的敏感性和 42.4%的特异性,低估了 17.0%的主要事件发生率。分诊助理的修订几乎没有改善紧急程度的分配。进一步考虑 OOH-PC 接触后的临床过程可以显著提高敏感性(89.4%)和特异性(61.9%)。
电话分诊胸痛的性能最多只能说是中等,具有可接受的安全性,但效率有限,即使包括 GP 的进一步检查也是如此。