Department of Global Health, Boston University School of Public Health, Boston University, Boston, MA, USA.
Department of Sociomedical Sciences, Mailman School of Public Health, Columbia University, New York, NY, USA.
BMC Health Serv Res. 2024 May 31;24(1):693. doi: 10.1186/s12913-024-10979-0.
Cervical cancer patients in Colombia have a lower likelihood of survival compared to breast cancer patients. In 1993, Colombia enrolled citizens in one of two health insurance regimes (contributory-private insurance and subsidized- public insurance) with fewer benefits in the subsidized regime. In 2008, the Constitutional Court required the Colombian government to unify services of both regimes by 2012. This study evaluated the impact of this insurance change on cervical cancer mortality before and after 2012.
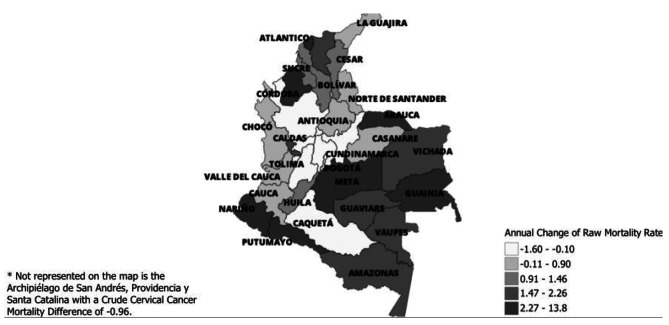
We accessed 24,491 cervical cancer mortality records for 2006-2020 from the vital statistics of Colombia's National Administrative Department of Statistics (DANE). We calculated crude mortality rates by health insurance type and departments (geopolitical division). Changes by department were analyzed by rate differences between 2006 and 2012 and 2013-2020, for each health insurance type. We analyzed trends using join-point regressions by health insurance and the two time-periods.
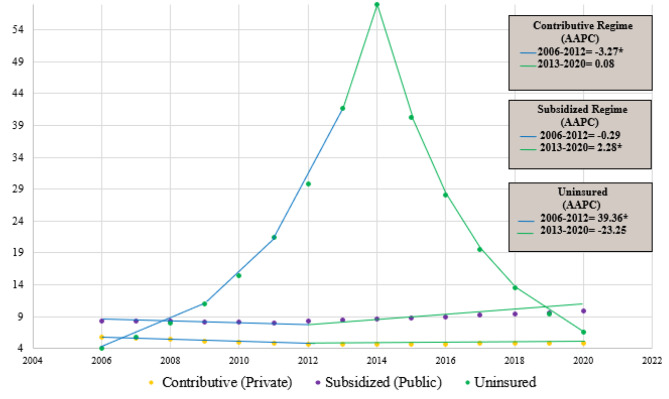
The contributory regime (private insurance) exhibited a significant decline in cervical cancer mortality from 2006 to 2012, characterized by a noteworthy average annual percentage change (AAPC) of -3.27% (P = 0.02; 95% CI [-5.81, -0.65]), followed by a marginal non-significant increase from 2013 to 2020 (AAPC 0.08%; P = 0.92; 95% CI [-1.63, 1.82]). In the subsidized regime (public insurance), there is a non-significant decrease in mortality between 2006 and 2012 (AAPC - 0.29%; P = 0.76; 95% CI [-2.17, 1.62]), followed by a significant increase from 2013 to 2020 (AAPC of 2.28%; P < 0.001; 95% CI [1.21, 3.36]). Examining departments from 2013 to 2020 versus 2006 to 2012, the subsidized regime showed fewer cervical cancer-related deaths in 5 out of 32 departments, while 6 departments had higher mortality. In 21 departments, mortality rates remained similar between both regimes.
Improvement of health benefits of the subsidized regime did not show a positive impact on cervical cancer mortality in women enrolled in this health insurance scheme, possibly due to unresolved administrative and socioeconomic barriers that hinder access to quality cancer screening and treatment.
与乳腺癌患者相比,哥伦比亚的宫颈癌患者的生存率较低。1993 年,哥伦比亚将公民纳入两种医疗保险制度之一(缴费制-私人保险和补贴制-公共保险),补贴制的福利较少。2008 年,宪法法院要求哥伦比亚政府在 2012 年前统一两个制度的服务。本研究评估了 2012 年前和 2012 年后这种保险变化对宫颈癌死亡率的影响。
我们从哥伦比亚国家统计署(DANE)的生命统计数据中获取了 2006 年至 2020 年的 24491 例宫颈癌死亡记录。我们按医疗保险类型和部门(地缘政治分区)计算了粗死亡率。对于每个医疗保险类型,我们通过 2006 年至 2012 年和 2013 年至 2020 年之间的发病率差异分析了部门的变化。我们通过医疗保险和两个时间段的联合点回归分析了趋势。
缴费制(私人保险)在 2006 年至 2012 年期间宫颈癌死亡率显著下降,具有显著的平均年百分比变化(AAPC)为-3.27%(P=0.02;95%CI [-5.81,-0.65]),随后 2013 年至 2020 年期间略有非显著增加(AAPC 0.08%;P=0.92;95%CI [-1.63,1.82])。在补贴制(公共保险)中,2006 年至 2012 年期间死亡率呈非显著下降(AAPC-0.29%;P=0.76;95%CI [-2.17,1.62]),随后 2013 年至 2020 年期间显著增加(AAPC 2.28%;P<0.001;95%CI [1.21,3.36])。从 2013 年至 2020 年与 2006 年至 2012 年相比,补贴制在 32 个部门中有 5 个部门宫颈癌相关死亡人数减少,而 6 个部门死亡率较高。在 21 个部门中,两种制度的死亡率保持相似。
补贴制的健康福利改善并未对参加该医疗保险计划的妇女的宫颈癌死亡率产生积极影响,这可能是由于未解决的行政和社会经济障碍阻碍了获得高质量的癌症筛查和治疗。