Department of Public and Occupational Health, Amsterdam UMC, Vrije Universiteit Amsterdam, Amsterdam Public Health Research Institute, P/O Box 7057, De Boelelaan 1117, Amsterdam, 1007 MB, The Netherlands.
Netherlands Institute for Health Services Research (Nivel), Utrecht, The Netherlands.
BMC Palliat Care. 2024 Jun 10;23(1):145. doi: 10.1186/s12904-024-01461-z.
Patient safety is crucial for quality of care. Preventable adverse events (AEs) occur in 1 of 20 patients in the hospital, but it is unknown whether this is different for patients with a condition relevant for palliative care. The majority of the limited available research on this topic is only focused on patients already receiving palliative care, and do not make comparisons with other patients at the end-of-life. We identified and compared the prevalence, preventability, nature and causes of AEs in patients with and without a condition relevant for palliative care.
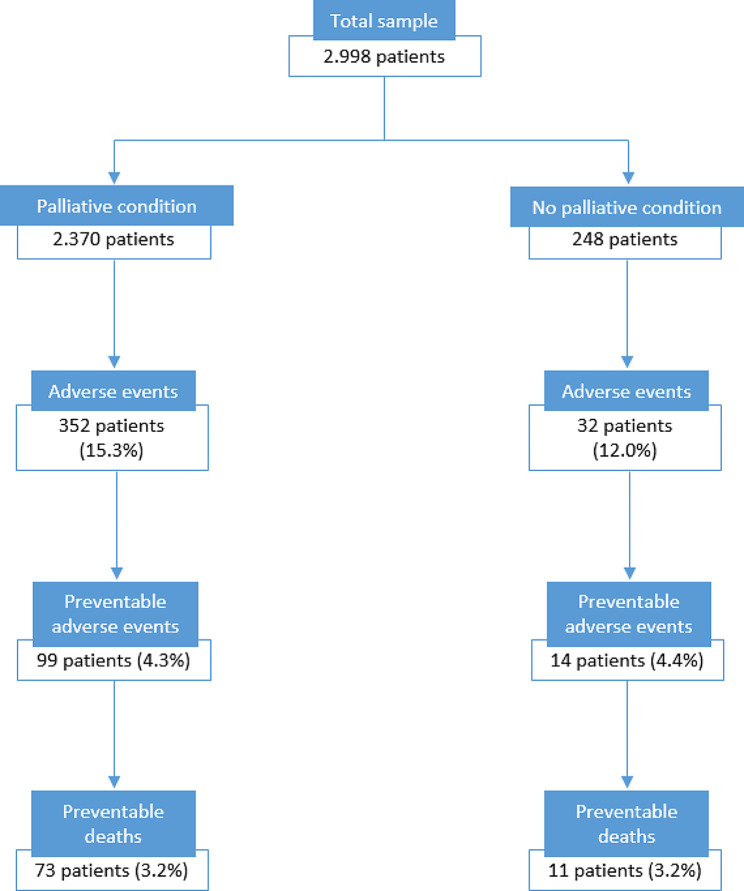
A nationwide retrospective record review study was performed in 20 Dutch hospitals. A total of 2,998 records of patients who died in hospital in 2019 was included. Records were reviewed for AEs. We identified two subgroups: patients with (n = 2,370) or without (n = 248) a condition relevant for palliative care through the selection method of Etkind (2017). Descriptive analyses were performed to calculate prevalence, nature, causes and prevention strategies. T-tests were performed to calculate differences between subgroups.
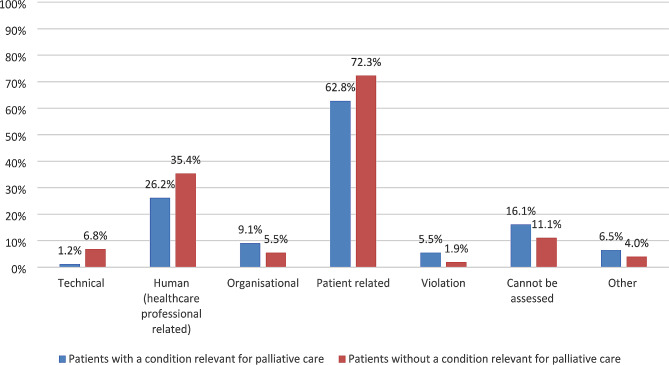
We found no significant differences between subgroups regarding AE prevalence, this was 15.3% in patients with a condition relevant for palliative care, versus 12.0% in patients without a condition relevant for palliative care (p = 0.148). Potentially preventable AE prevalence was 4.3% versus 4.4% (p = 0.975). Potentially preventable death prevalence in both groups was 3.2% (p = 0.938). There were differences in the nature of AEs: in patients with a condition relevant for palliative care this was mostly related to medication (33.1%), and in patients without a condition relevant for palliative care to surgery (50.8%). In both subgroups in the majority of AEs a patient related cause was identified. For the potentially preventable AEs in both subgroups the two most important prevention strategies as suggested by the medical reviewers were reflection and evaluation and quality assurance.
Patient safety risks appeared to be equally prevalent in both subgroups. The nature of AEs does differ between subgroups: medication- versus surgery-related, indicating that tailored safety measures are needed. Recommendations for practice are to focus on reflecting on AEs, complemented with case evaluations.
患者安全对于医疗质量至关重要。在医院中,每 20 名患者中就会发生 1 例可预防的不良事件(AE),但尚不清楚这是否与接受姑息治疗相关的患者不同。关于这一主题的有限研究大多仅关注已经接受姑息治疗的患者,而没有与生命末期的其他患者进行比较。我们确定并比较了患有和不患有姑息治疗相关疾病的患者中 AE 的发生率、可预防性、性质和原因。
在 20 家荷兰医院进行了一项全国性的回顾性病历审查研究。共纳入了 2019 年在医院死亡的 2998 名患者的病历。审查病历以确定 AE。我们通过 Etkind(2017)的选择方法确定了两个亚组:患有(n=2370)或不患有(n=248)姑息治疗相关疾病的患者。进行描述性分析以计算发生率、性质、原因和预防策略。进行 t 检验以计算亚组之间的差异。
我们发现亚组之间 AE 发生率没有显著差异,患有姑息治疗相关疾病的患者为 15.3%,而不患有姑息治疗相关疾病的患者为 12.0%(p=0.148)。潜在可预防 AE 的发生率为 4.3%与 4.4%(p=0.975)。两个组中潜在可预防的死亡发生率均为 3.2%(p=0.938)。AE 的性质存在差异:在患有姑息治疗相关疾病的患者中,主要与药物治疗有关(33.1%),而在不患有姑息治疗相关疾病的患者中,主要与手术有关(50.8%)。在两个亚组中,大多数 AE 都确定了与患者相关的原因。对于两个亚组中的潜在可预防 AE,医学审查员建议的两个最重要的预防策略是反思和评估以及质量保证。
患者安全风险在两个亚组中似乎同样普遍。AE 的性质在亚组之间存在差异:与药物治疗相关与手术相关,这表明需要有针对性的安全措施。实践建议是专注于对 AE 进行反思,并辅以病例评估。