Valentine Michael J, Hayat Fakhar, Kayastha Ankur, Newsome-Cuby Takara R, Nguyen Anh Thu N, AlDallal Usama, Ismail Mohamed
Medical School, Kansas City University, Kansas City, USA.
Neurosurgery, King Hamad University Hospital, Al Sayh, BHR.
Cureus. 2024 May 12;16(5):e60141. doi: 10.7759/cureus.60141. eCollection 2024 May.
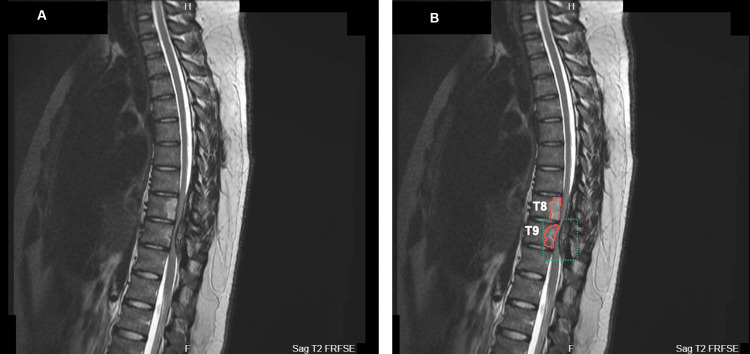
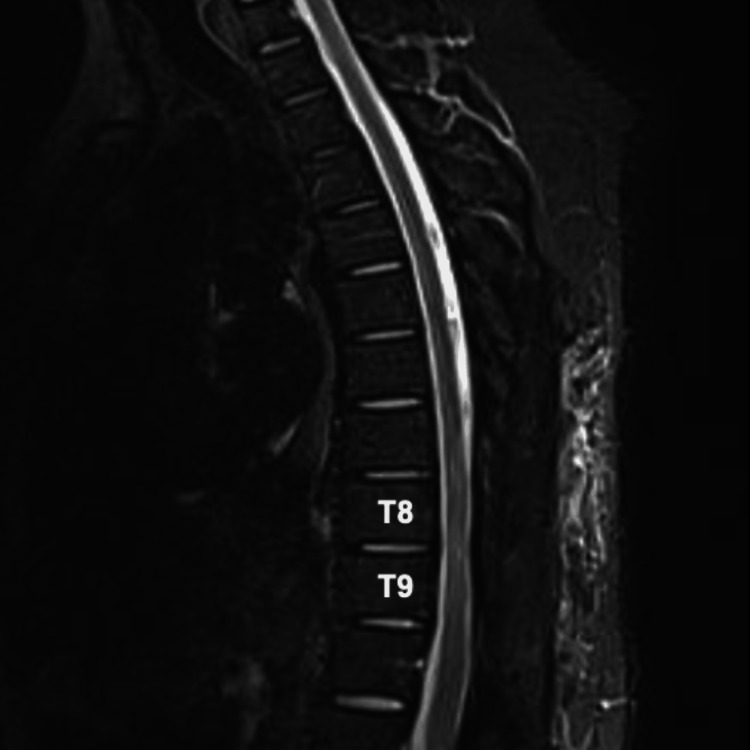
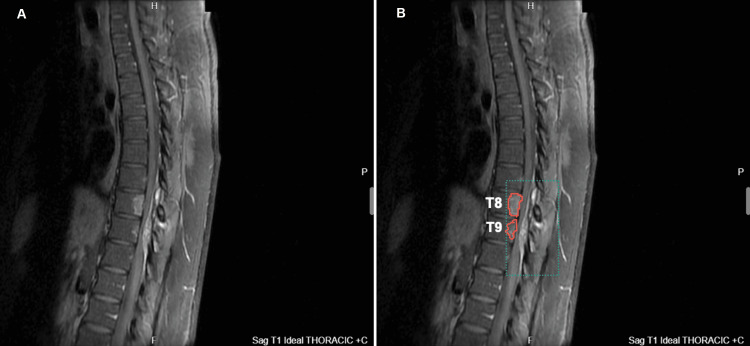
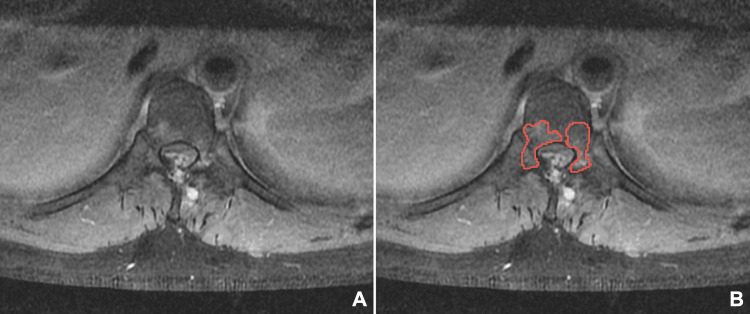
Spinal cord compression is a neurosurgical emergency. Symptoms of this disorder are highlighted as back pain, ambulatory difficulties, and bladder/bowel incontinence. Diagnostic imaging is not indicated in many circumstances of nonspecific back pain; however, the addition of neurologic deficits in the setting of back pain justifies radiologic imaging. Various pathologies can cause constriction of the spinal cord due to the delicate nature of spinal cord anatomy. Etiologies may include trauma, neoplasms, and infections. In this report, we present an unusual case of a 31-year-old male who presented to the emergency department with a history of chronic back pain accompanied by neurological deficits, ataxia, and bladder dysfunction. Contrast-enhanced MRI imaging heightened the suspicion of a neoplastic etiology; however, neuropathology revealed a non-neoplastic nature with abnormal lymphohistiocytic infiltrate suspicious for Langerhans cell histiocytosis or infectious etiology. A second opinion was provided by Mayo Clinic Laboratories, resulting in the definitive conclusion that the mass was non-neoplastic and tested negative for SD1a and Langerhin, biomarkers used to diagnose Langerhans cell histiocytosis. This unusual non-neoplastic lesion exemplifies one of many diverse and multifaceted pathologies that can precipitate spinal cord compression. Additionally, these findings underscore the importance of considering both neoplastic and non-neoplastic causes in the differential diagnosis of spinal cord compression, thereby enhancing clinical vigilance and improving patient outcomes for underlying spinal conditions.
脊髓压迫是一种神经外科急症。这种疾病的症状表现为背痛、行走困难以及膀胱/肠道失禁。在许多非特异性背痛的情况下,并不需要进行诊断性影像学检查;然而,在背痛的基础上出现神经功能缺损则有理由进行放射学成像检查。由于脊髓解剖结构的精细性,多种病理情况都可能导致脊髓受压。病因可能包括创伤、肿瘤和感染。在本报告中,我们介绍了一例不同寻常的病例,一名31岁男性因慢性背痛病史并伴有神经功能缺损、共济失调和膀胱功能障碍而就诊于急诊科。增强磁共振成像(MRI)检查增加了肿瘤性病因的怀疑;然而,神经病理学检查显示为非肿瘤性性质,伴有异常的淋巴组织细胞浸润,怀疑为朗格汉斯细胞组织细胞增多症或感染性病因。梅奥诊所实验室提供了第二种意见,最终得出结论,该肿块为非肿瘤性,并且用于诊断朗格汉斯细胞组织细胞增多症的生物标志物SD1a和Langerhin检测呈阴性。这种不同寻常的非肿瘤性病变体现了众多可能导致脊髓压迫的多样且复杂的病理情况之一。此外,这些发现强调了在脊髓压迫的鉴别诊断中考虑肿瘤性和非肿瘤性病因的重要性,从而提高对潜在脊柱疾病的临床警惕性并改善患者预后。