Melanoma Institute Australia, The University of Sydney, Sydney, New South Wales, Australia.
Faculty of Medicine and Health, The University of Sydney, Sydney, New South Wales, Australia.
Nat Med. 2024 Sep;30(9):2540-2548. doi: 10.1038/s41591-024-03077-5. Epub 2024 Jun 21.
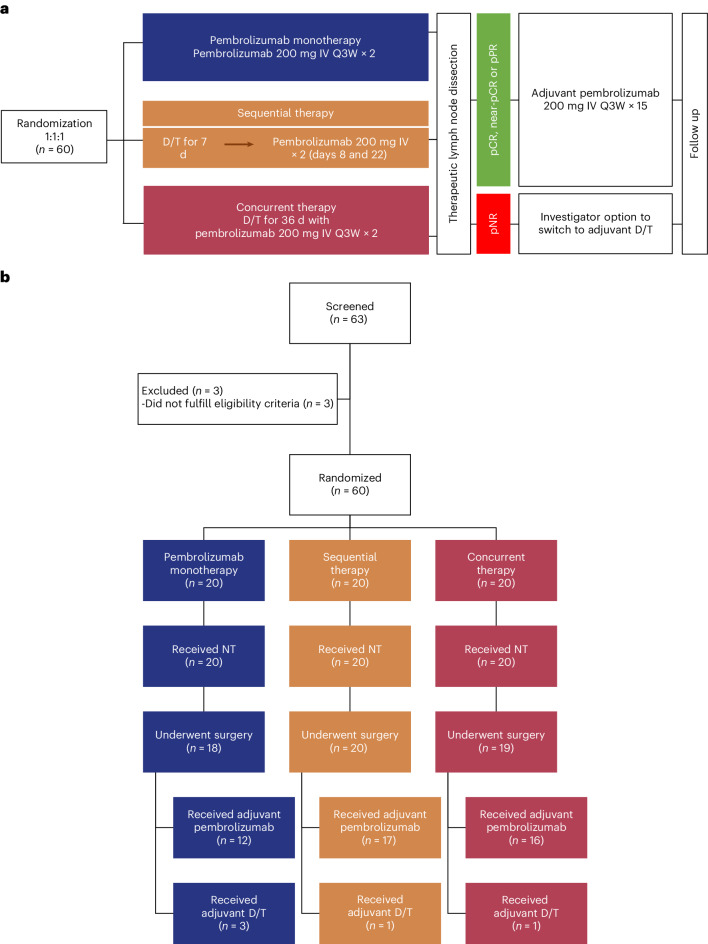
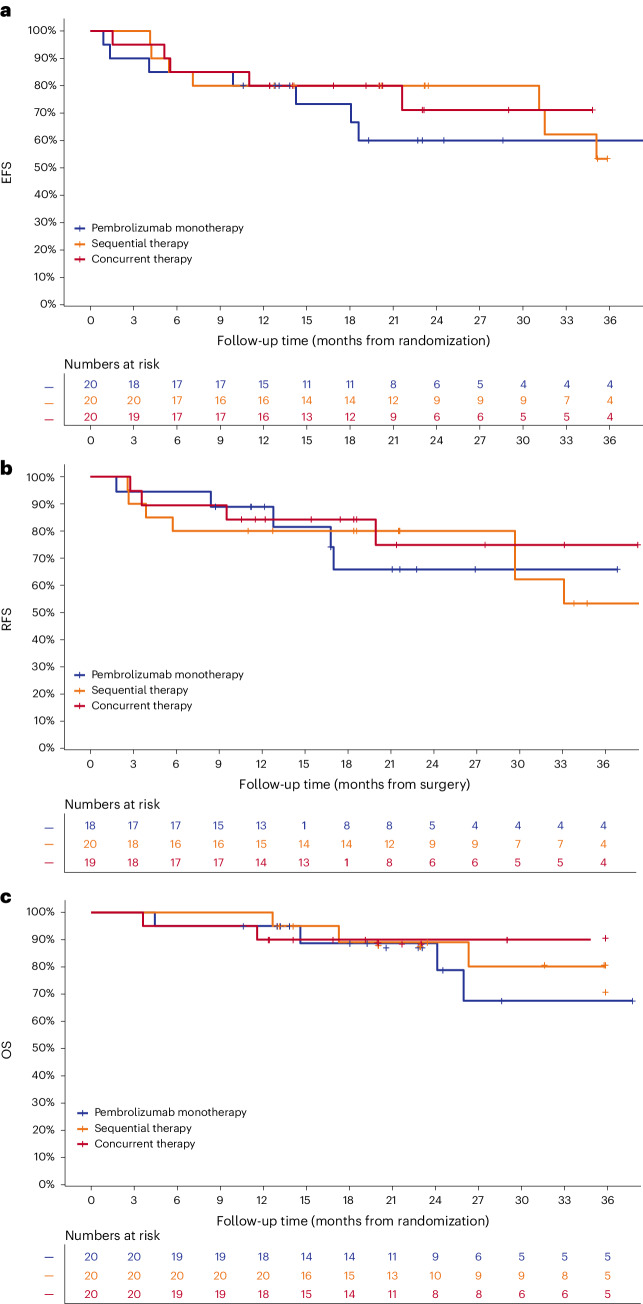
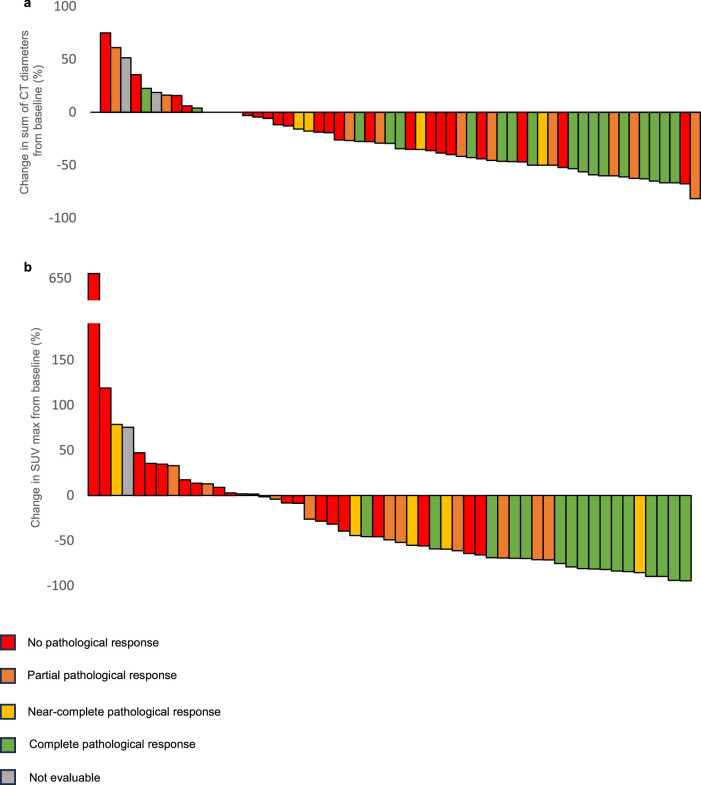
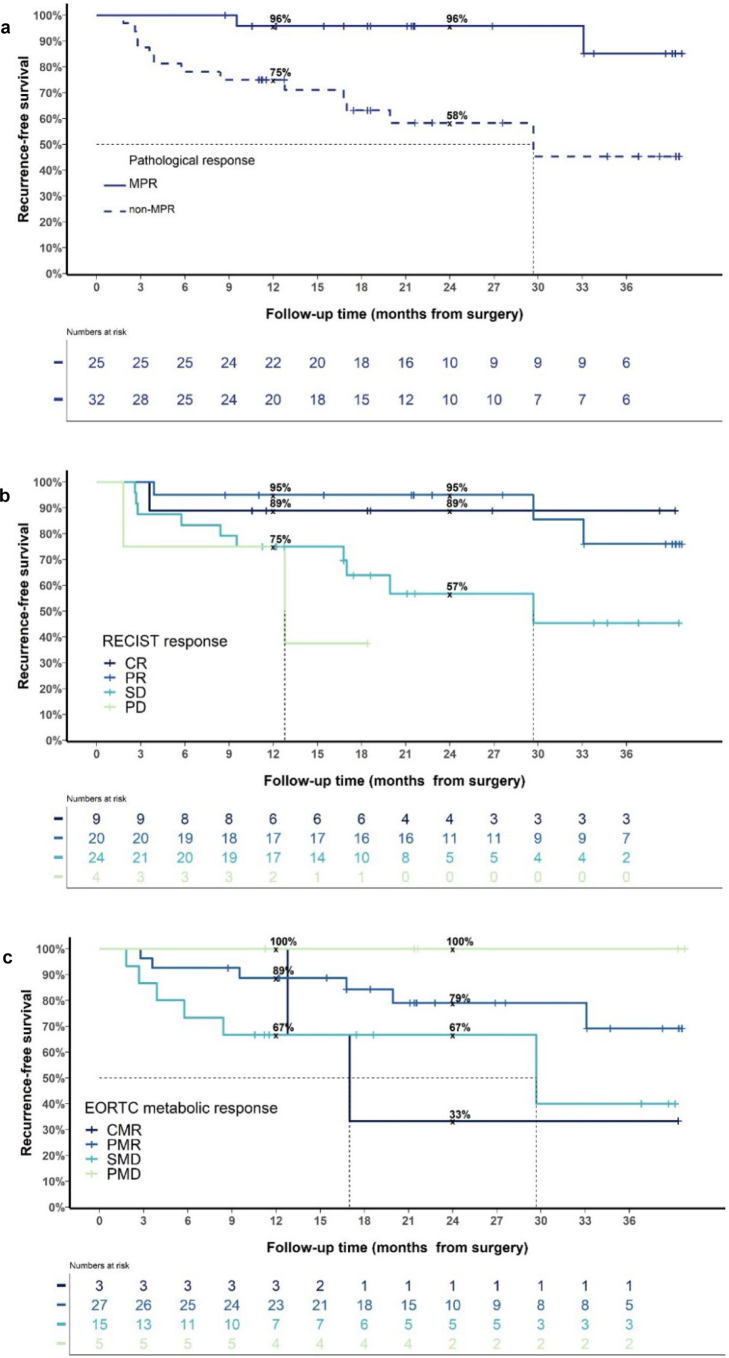
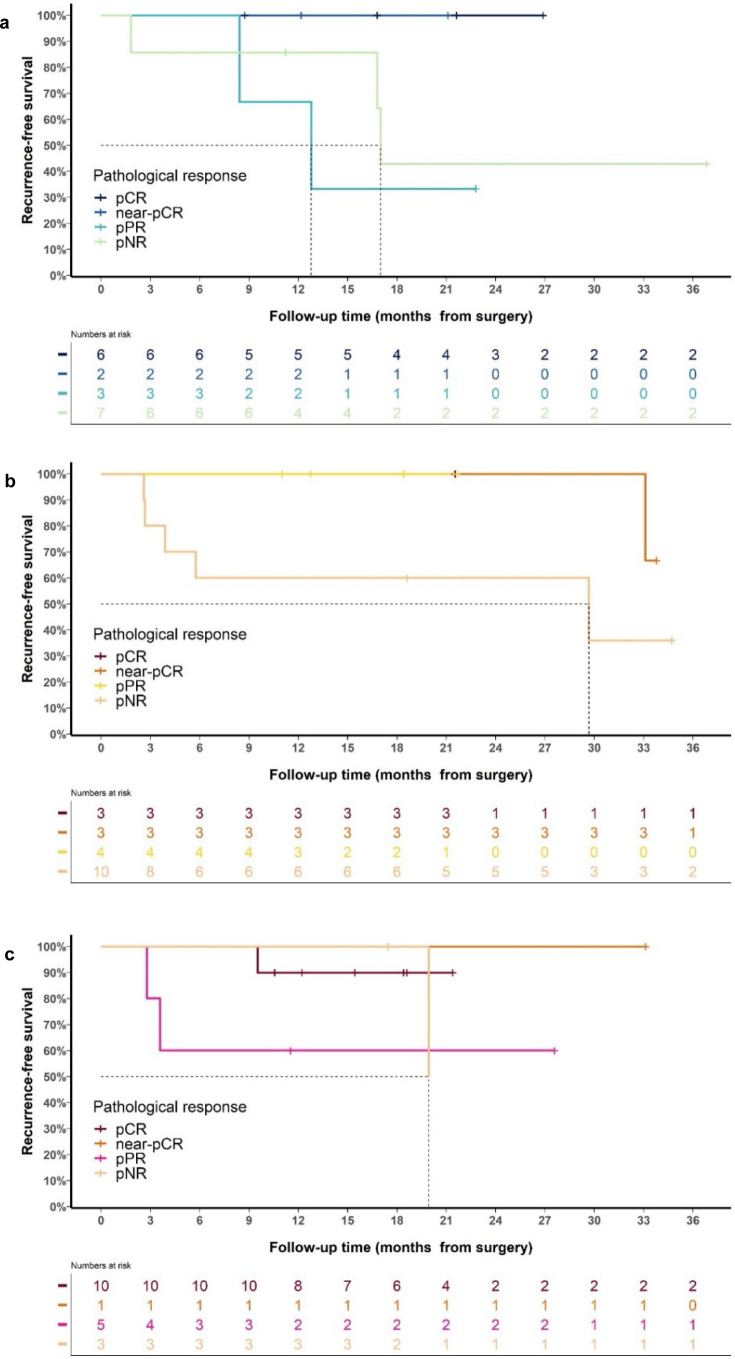
Immune checkpoint inhibitors and BRAF-targeted therapy each improve survival in melanoma. Immune changes early during targeted therapy suggest the mechanisms of each drug class could work synergistically. In the non-comparative, randomized, phase 2 NeoTrio trial, we investigated whether targeted therapy could boost the proportion of patients achieving long-term recurrence-free survival with neoadjuvant immunotherapy in resectable stage III BRAF-mutant melanoma. Sixty patients (42% females) were randomized to pembrolizumab alone (n = 20), sequential therapy (dabrafenib plus trametinib followed by pembrolizumab; n = 20) or concurrent (triple) therapy (n = 20), followed by surgery and adjuvant therapy. The primary outcome was pathological response; secondary outcomes included radiographic response, recurrence-free survival, overall survival, surgical outcomes, peripheral blood and tumor analyses and safety. The pathological response rate was 55% (11/20; including six pathological complete responses (pCRs)) with pembrolizumab, 50% (10/20; three pCRs) with sequential therapy and 80% (16/20; ten pCRs) with concurrent therapy, which met the primary outcome in each arm. Treatment-related adverse events affected 75-100% of patients during neoadjuvant treatment, with seven early discontinuations (all in the concurrent arm). At 2 years, event-free survival was 60% with pembrolizumab, 80% with sequential therapy and 71% with concurrent therapy. Recurrences after major pathological response were more common in the targeted therapy arms, suggesting a reduction in response 'quality' when targeted therapy is added to neoadjuvant immunotherapy. Risking the curative potential of immunotherapy in melanoma cannot be justified. Pending longer follow-up, we suggest that immunotherapy and targeted therapy should not be combined in the neoadjuvant setting for melanoma. ClinicalTrials.gov registration: NCT02858921 .
免疫检查点抑制剂和 BRAF 靶向治疗均可改善黑色素瘤患者的生存率。靶向治疗早期的免疫变化表明,这两类药物的作用机制可能具有协同作用。在非对照、随机、Ⅱ期 Neotrio 试验中,我们研究了在可切除 III 期 BRAF 突变黑色素瘤患者中,靶向治疗是否能提高新辅助免疫治疗使患者长期无复发生存率的比例。60 例患者(42%为女性)被随机分配至帕博利珠单抗单药组(n=20)、序贯治疗组(达布拉非尼加曲美替尼序贯帕博利珠单抗,n=20)或同步(三联)治疗组(n=20),随后行手术和辅助治疗。主要终点是病理缓解;次要终点包括影像学缓解、无复发生存率、总生存率、手术结局、外周血和肿瘤分析以及安全性。帕博利珠单抗组的病理缓解率为 55%(20 例中有 11 例,包括 6 例病理完全缓解[pCR]),序贯治疗组为 50%(20 例中有 10 例,3 例 pCR),同步治疗组为 80%(20 例中有 16 例,10 例 pCR),各治疗组均达到了主要终点。新辅助治疗期间,治疗相关不良事件影响了 75-100%的患者,有 7 例早期停药(均在同步治疗组)。2 年时,帕博利珠单抗组的无事件生存率为 60%,序贯治疗组为 80%,同步治疗组为 71%。在主要病理缓解后复发的情况在靶向治疗组更常见,这表明当靶向治疗与新辅助免疫治疗联合应用时,会降低反应的“质量”。冒着黑色素瘤免疫治疗的治愈潜力的风险是不合理的。在更长时间的随访结果出来之前,我们建议新辅助治疗黑色素瘤时不应将免疫治疗和靶向治疗联合应用。临床试验注册:NCT02858921。