Orkaby Ariela R, Goyal Parag, Charest Brian, Qazi Saadia, Sheikh Shamlan, Shah Sanjiv, Gaziano J Michael, Djousse Luc, Gagnon David, Joseph Jacob
New England Geriatric Research, Education, and Clinical Center (GRECC), VA Boston Healthcare System, Boston, Massachusetts, USA.
Massachusetts Veterans Epidemiology Research and Information Center (MAVERIC), VA Boston Healthcare System, Boston, Massachusetts, USA.
JACC Adv. 2024 Feb 20;3(4):100869. doi: 10.1016/j.jacadv.2024.100869. eCollection 2024 Apr.
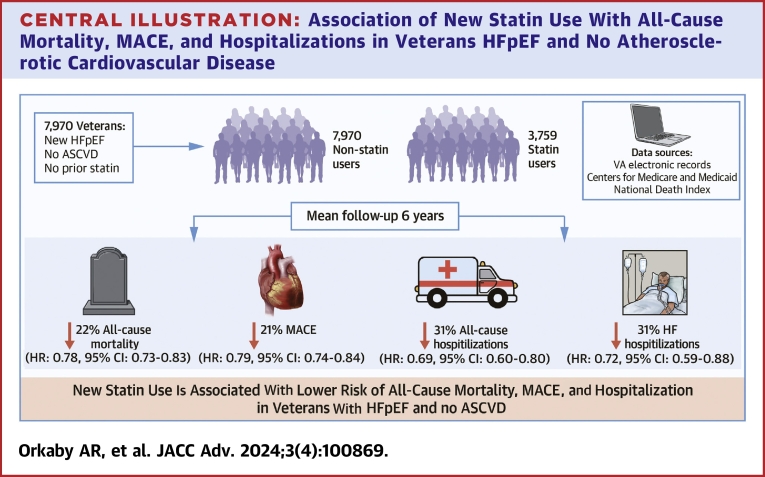
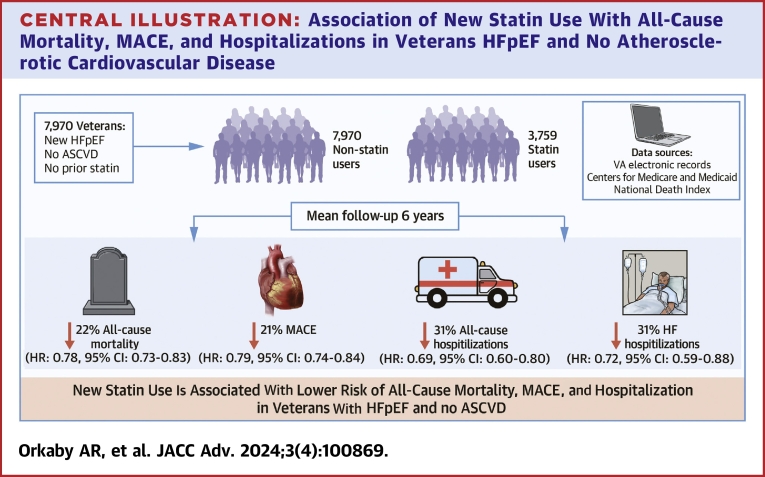
Statins are highly effective for primary prevention of atherosclerotic cardiovascular disease (ASCVD) and mortality. Data on the benefit of statins in adults with heart failure with preserved ejection fraction (HFpEF) and without ASCVD are limited.
The purpose of this study was to determine whether statins are associated with a lower risk of mortality and major adverse cardiovascular events (MACE) in HFpEF.
Veterans Health Administration data from 2002 to 2016, linked to Medicare and Medicaid claims and pharmaceutical data, were collected. Patients had a new HFpEF diagnosis and no known ASCVD or prior statin use at baseline. Cox proportional hazards models were fit to evaluate the association of new statin use with outcomes (all-cause mortality and MACE). Propensity score overlap weighting (PSW) was used to balance baseline characteristics.
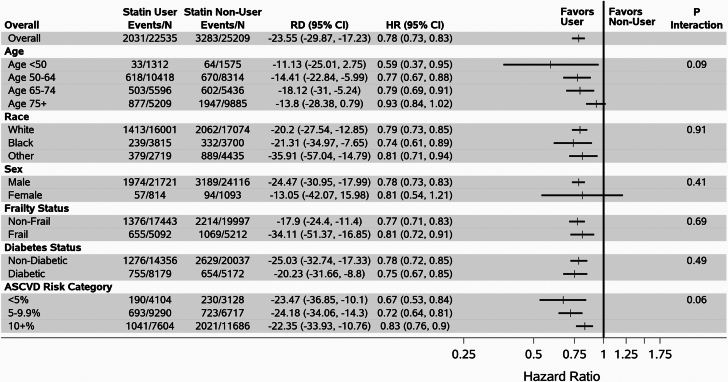
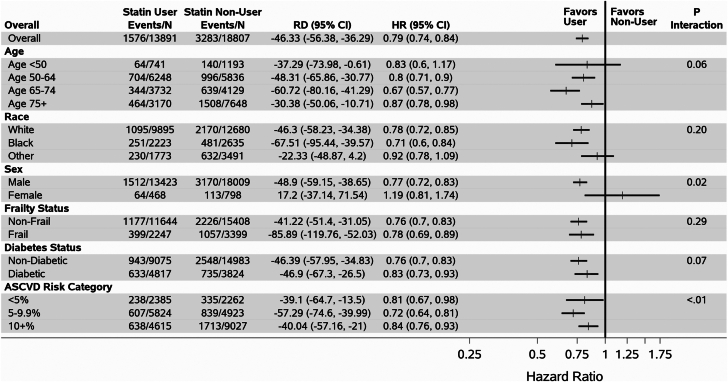
Among 7,970 Veterans, 47% initiated a statin over a mean 6.0-year follow-up. At HFpEF diagnosis, mean age was 69 ± 12 years, 96% were male, 67% were White, 14% were Black, and mean EF was 60% ± 6%. Before PSW, statin users were younger with more prevalent metabolic syndrome, arthritis, and other chronic conditions. All characteristics were balanced after PSW. There were 5,314 deaths and 4,859 MACE events. After PSW, the hazard for all-cause mortality for statin users vs nonusers was 22% lower (HR: 0.78; 95% CI: 0.73-0.83). The HR for MACE was 0.79 (95% CI: 0.74-0.84), 0.69 (95% CI: 0.60-0.80) for all-cause hospitalization, and 0.72 (95% CI: 0.59-0.88) for HF hospitalization.
New statin use was associated with reduced all-cause mortality, MACE, and hospitalization in Veterans with HFpEF without prevalent ASCVD.
他汀类药物对动脉粥样硬化性心血管疾病(ASCVD)的一级预防及降低死亡率非常有效。关于他汀类药物对射血分数保留的心力衰竭(HFpEF)且无ASCVD的成年人的益处的数据有限。
本研究旨在确定他汀类药物是否与HFpEF患者较低的死亡风险和主要不良心血管事件(MACE)相关。
收集了2002年至2016年退伍军人健康管理局的数据,并与医疗保险和医疗补助索赔以及药品数据相链接。患者在基线时被新诊断为HFpEF,且无已知的ASCVD或既往他汀类药物使用史。采用Cox比例风险模型评估新使用他汀类药物与结局(全因死亡率和MACE)之间的关联。倾向评分重叠加权(PSW)用于平衡基线特征。
在7970名退伍军人中,47%在平均6.0年的随访期间开始使用他汀类药物。在HFpEF诊断时,平均年龄为69±12岁,96%为男性,67%为白人,14%为黑人,平均射血分数为60%±6%。在PSW之前,他汀类药物使用者更年轻,代谢综合征、关节炎和其他慢性病更为普遍。PSW后所有特征均达到平衡。有5314例死亡和4859例MACE事件。PSW后,他汀类药物使用者与非使用者相比,全因死亡率风险降低22%(HR:0.78;95%CI:0.73-0.83)。MACE的HR为0.79(95%CI:0.74-0.84),全因住院的HR为0.69(95%CI:0.60-0.80),HF住院的HR为0.72(95%CI:0.59-0.88)。
新使用他汀类药物与无普遍ASCVD的HFpEF退伍军人的全因死亡率、MACE和住院率降低相关。