Department of Hematology-Oncology, Maroone Cancer Center, Cleveland Clinic Florida, Weston.
Department of Internal Medicine, Advent Health Sebring, Sebring, Florida.
JAMA Netw Open. 2024 Jul 1;7(7):e2419142. doi: 10.1001/jamanetworkopen.2024.19142.
Among patients with metastatic colorectal cancer (mCRC), data are limited on disparate biomarker testing and its association with clinical outcomes on a national scale.
To evaluate the socioeconomic and demographic inequities in microsatellite instability (MSI) and KRAS biomarker testing among patients with mCRC and to explore the association of testing with overall survival (OS).
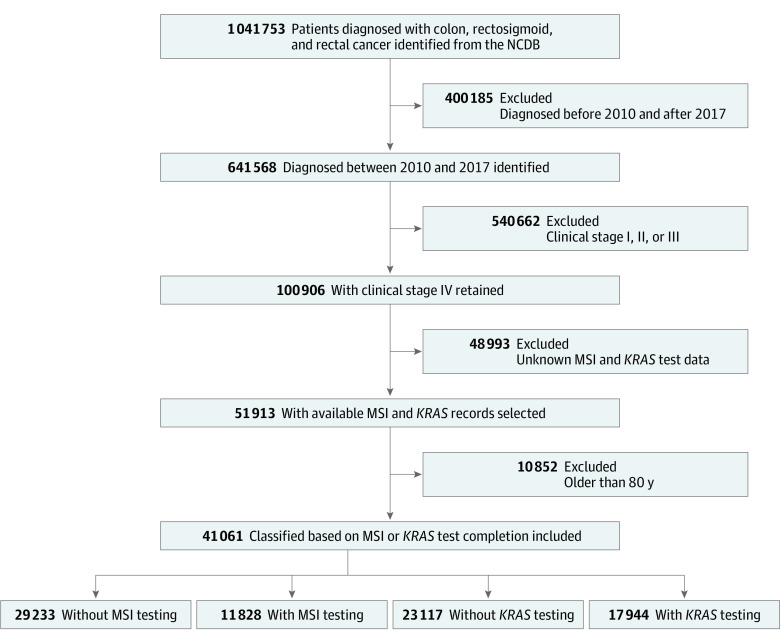
DESIGN, SETTING, AND PARTICIPANTS: This cohort study, conducted between November 2022 and March 2024, included patients who were diagnosed with mCRC between January 1, 2010, and December 31, 2017. The study obtained data from the National Cancer Database, a hospital-based cancer registry in the US. Patients with mCRC and available information on biomarker testing were included. Patients were classified based on whether they completed or did not complete MSI or KRAS tests.
Demographic and socioeconomic factors, such as age, race, ethnicity, educational level in area of residence, median household income, insurance type, area of residence, facility type, and facility location were evaluated.
The main outcomes were MSI and KRAS testing between the date of diagnosis and the date of first-course therapy. Univariable and multivariable logistic regressions were used to identify the relevant factors in MSI and KRAS testing. The OS outcomes were also evaluated.
Among the 41 061 patients included (22 362 males [54.5%]; mean [SD] age, 62.3 [10.1] years; 17.3% identified as Black individuals, 78.0% as White individuals, 4.7% as individuals of other race, with 6.5% Hispanic or 93.5% non-Hispanic ethnicity), 28.8% underwent KRAS testing and 43.7% received MSI testing. A significant proportion of patients had Medicare insurance (43.6%), received treatment at a comprehensive community cancer program (40.5%), and lived in an area with lower educational level (51.3%). Factors associated with a lower likelihood of MSI testing included age of 70 to 79 years (relative risk [RR], 0.70; 95% CI, 0.66-0.74; P < .001), treatment at a community cancer program (RR, 0.74; 95% CI, 0.70-0.79; P < .001), rural residency (RR, 0.80; 95% CI, 0.69-0.92; P < .001), lower educational level in area of residence (RR, 0.84; 95% CI, 0.79-0.89; P < .001), and treatment at East South Central facilities (RR, 0.67; 95% CI, 0.61-0.73; P < .001). Similar patterns were observed for KRAS testing. Survival analysis showed modest OS improvement in patients with MSI testing (hazard ratio, 0.93; 95% CI, 0.91-0.96; P < .001). The median (IQR) follow-up time for the survival analysis was 13.96 (3.71-29.34) months.
This cohort study of patients with mCRC found that older age, community-setting treatment, lower educational level in area of residence, and treatment at East South Central facilities were associated with a reduced likelihood of MSI and KRAS testing. Highlighting the sociodemographic-based disparities in biomarker testing can inform the development of strategies that promote equity in cancer care and improve outcomes for underserved populations.
重要性:在转移性结直肠癌(mCRC)患者中,有关不同生物标志物检测及其与全国范围内临床结局的关联的数据有限。
目的:评估 mCRC 患者微卫星不稳定性(MSI)和 KRAS 生物标志物检测中的社会经济和人口统计学差异,并探讨检测与总生存(OS)的关联。
设计、地点和参与者:这是一项队列研究,于 2022 年 11 月至 2024 年 3 月进行,纳入了 2010 年 1 月 1 日至 2017 年 12 月 31 日期间诊断为 mCRC 的患者。该研究从美国基于医院的癌症登记处国家癌症数据库中获取数据。纳入了有 mCRC 且有生物标志物检测信息的患者。患者根据是否完成或未完成 MSI 或 KRAS 检测进行分类。
暴露:评估了人口统计学和社会经济因素,如年龄、种族、民族、居住地的教育水平、家庭收入中位数、保险类型、居住地、医疗机构类型和医疗机构位置。
主要结果和测量:主要结果是在诊断日期和首次治疗日期之间进行 MSI 和 KRAS 检测。使用单变量和多变量逻辑回归来确定 MSI 和 KRAS 检测中的相关因素。还评估了 OS 结果。
结果:在纳入的 41061 名患者中(22362 名男性[54.5%];平均[标准差]年龄 62.3[10.1]岁;17.3%为黑人个体,78.0%为白人个体,4.7%为其他种族个体,6.5%为西班牙裔或 93.5%为非西班牙裔),28.8%的患者接受了 KRAS 检测,43.7%的患者接受了 MSI 检测。相当一部分患者拥有医疗保险(43.6%),在综合性社区癌症项目中接受治疗(40.5%),居住在教育水平较低的地区(51.3%)。与 MSI 检测可能性降低相关的因素包括年龄 70 至 79 岁(相对风险[RR],0.70;95%CI,0.66-0.74;P<0.001)、在社区癌症项目中接受治疗(RR,0.74;95%CI,0.70-0.79;P<0.001)、农村居住(RR,0.80;95%CI,0.69-0.92;P<0.001)、居住地教育水平较低(RR,0.84;95%CI,0.79-0.89;P<0.001)和在东中南部地区的医疗机构接受治疗(RR,0.67;95%CI,0.61-0.73;P<0.001)。KRAS 检测也存在类似的模式。生存分析显示,MSI 检测患者的 OS 有适度改善(危险比,0.93;95%CI,0.91-0.96;P<0.001)。生存分析的中位(IQR)随访时间为 13.96(3.71-29.34)个月。
结论和相关性:这项针对 mCRC 患者的队列研究发现,年龄较大、社区环境下的治疗、居住地教育水平较低和东中南部地区医疗机构的治疗与 MSI 和 KRAS 检测的可能性降低有关。强调生物标志物检测中的社会人口统计学差异,可以为制定促进癌症护理公平的策略提供信息,并改善服务不足人群的结局。