Department of Pediatric Metabolism, Ankara Etlik City Hospital Health Complex Children's Hospital, Ankara, Turkey.
Department of Pediatric Intensive Care Medicine, Ankara Etlik City Hospital, Ankara, Turkey.
BMC Nephrol. 2024 Jul 8;25(1):217. doi: 10.1186/s12882-024-03656-1.
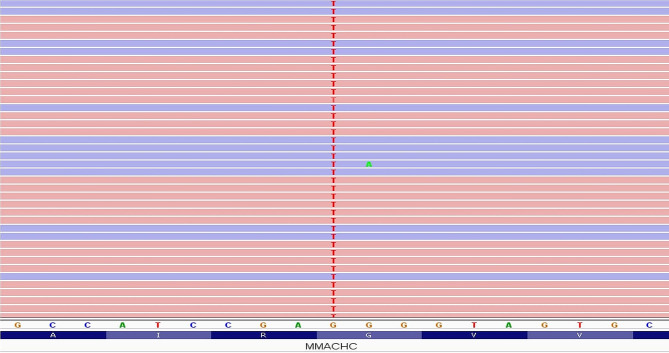
The etiology of nephrotic syndrome can vary, with underlying metabolic diseases being a potential factor. Cobalamin C (cblC) defect is an autosomal recessive inborn error of metabolism caused by mutations in the MMACHC gene, resulting in impaired vitamin B12 processing. While cblC defect typically manifests with hematological and neurological symptoms, renal involvement is increasingly recognized but remains rare.
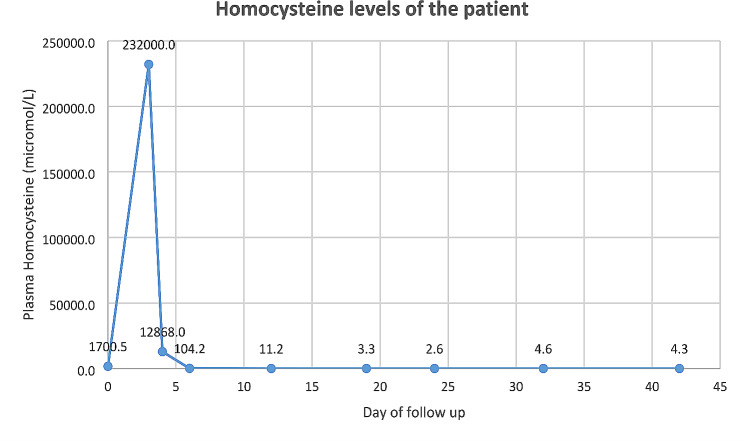
We describe a 7-month-old male patient presenting with fatigue and edema. His first laboratory findings showed anemia, thrombocytopenia, hypoalbuminemia and proteinuria and further examinations reveals hemolysis in peripheric blood smear. During his follow up respiratory distress due to pleural effusion in the right hemithorax was noticed. And fluid leakage to the third spaces supported nephrotic syndrome diagnosis. The patient's condition deteriorated, leading to intensive care admission due to, hypertensive crisis, and respiratory distress. High total plasma homocysteine and low methionine levels raised suspicion of cobalamin metabolism disorders. Genetic testing confirmed biallelic MMACHC gene mutations, establishing the diagnosis of cblC defect. Treatment with hydroxycobalamin, folic acid, and betaine led to remarkable clinical improvement.
DISCUSSION/CONCLUSION: This case underscores the significance of recognizing metabolic disorders like cblC defect in atypical presentations of nephrotic syndrome. Early diagnosis and comprehensive management are vital to prevent irreversible renal damage. While cblC defects are more commonly associated with atypical hemolytic uremic syndrome, this case highlights the importance of considering cobalamin defects in the differential diagnosis of nephrotic syndrome, especially when associated with accompanying findings such as hemolysis. Our case, which has one of the highest homocysteine levels reported in the literature, emphasizes this situation again.
肾病综合征的病因多种多样,潜在的代谢性疾病是一个潜在因素。钴胺素 C(cblC)缺陷是一种常染色体隐性遗传性代谢紊乱,由 MMACHC 基因突变引起,导致维生素 B12 处理受损。虽然 cblC 缺陷通常表现为血液学和神经系统症状,但越来越多的人认识到肾脏受累,但仍然很少见。
我们描述了一名 7 个月大的男性患者,表现为疲劳和水肿。他的首次实验室检查结果显示贫血、血小板减少、低白蛋白血症和蛋白尿,进一步检查发现外周血涂片有溶血。在随访过程中,注意到右侧胸腔积液压迫性呼吸困难。液体漏入第三间隙支持肾病综合征的诊断。患者病情恶化,因高血压危象和呼吸窘迫而需要入住重症监护病房。高总血浆同型半胱氨酸和低蛋氨酸水平提示钴胺素代谢紊乱。基因检测证实存在 MMACHC 基因的双等位基因突变,确立了 cblC 缺陷的诊断。用羟钴胺、叶酸和甜菜碱治疗后,临床症状显著改善。
讨论/结论:本病例强调了在非典型肾病综合征表现中识别代谢紊乱(如 cblC 缺陷)的重要性。早期诊断和综合管理对于预防不可逆转的肾损伤至关重要。虽然 cblC 缺陷更常见于非典型溶血性尿毒症综合征,但本病例强调了在肾病综合征的鉴别诊断中考虑钴胺素缺陷的重要性,特别是当伴有溶血等伴随发现时。我们的病例再次强调了这一点,其同型半胱氨酸水平是文献中报告的最高水平之一。