Pediatric Nephrology, University of Texas Southwestern Medical Center, Dallas, TX, USA.
Pediatric Genetics and Metabolism, University of Texas Southwestern Medical Center, Dallas, TX, USA.
Pediatr Nephrol. 2022 Jun;37(6):1415-1418. doi: 10.1007/s00467-021-05372-6. Epub 2021 Dec 2.
Cobalamin C (cblC), a vitamin B12 processing protein, plays a crucial role in metabolism for the conversion of homocysteine to methionine and methylmalonyl-CoA to succinyl-CoA. CblC deficiency, an inborn error of cobalamin processing, is a rare cause of atypical hemolytic-uremic syndrome (aHUS) and results in hyperhomocysteinemia and methylmalonic aciduria. Both substances are thought to contribute to thrombotic microangiopathy (TMA) in cblC deficiency patients. However, the roles of homocysteine and methylmalonic acid (MMA) in these patients remain unclear. We want to shed more light on the contributions of homocysteine and MMA levels as contributing factors for thrombotic microangiopathy (TMA)/aHUS by a follow-up of a cblC deficiency patient over 6 years.
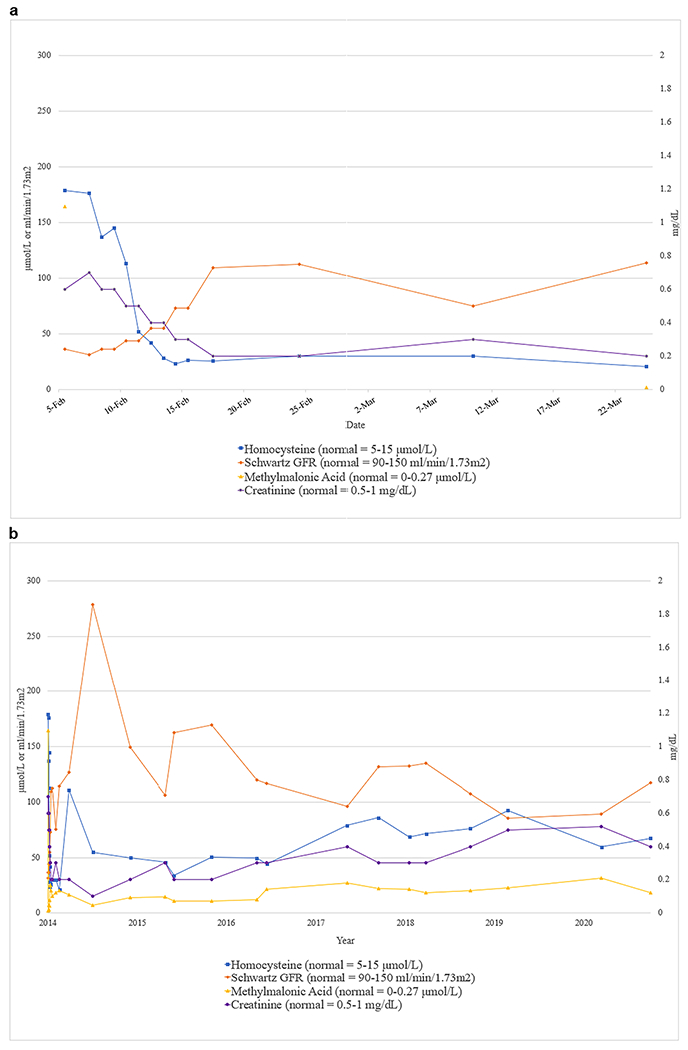
A 27-day-old Hispanic female presented with abnormal C3-carnitine on her newborn screen, poor feeding, decreased activity, and oligouria. She was diagnosed with cblC deficiency after laboratory results revealed elevated serum homocysteine, and serum MMA along with genetic testing showing a homozygous pathogenic frameshift variant in MMACHC. The patient developed aHUS and acute kidney injury (AKI), which resolved after appropriate therapy. Over 6 years, she continued to have normal kidney function with no thrombocytopenia despite persistently elevated homocysteine and MMA levels.
We question the roles of homocysteine and MMA as causative of aHUS/TMA in cblC deficiency as they remained elevated during follow-up but did not result in aHUS/TMA or AKI. Hyperhomocysteinemia and/or MMA caused by other metabolic diseases do not result in aHUS/TMA or AKI. This suggests that other nephrotoxic factors may trigger aHUS/TMA in cblC patients.
钴胺素 C(cblC)是一种维生素 B12 加工蛋白,在将同型半胱氨酸转化为蛋氨酸和甲基丙二酰辅酶 A 转化为琥珀酰辅酶 A 的代谢中起着至关重要的作用。钴胺素 C 缺乏症是一种罕见的钴胺素加工缺陷,是非典型溶血尿毒综合征(aHUS)的一个原因,并导致高同型半胱氨酸血症和甲基丙二酸尿症。这两种物质都被认为是 cblC 缺乏症患者血栓性微血管病(TMA)的原因。然而,同型半胱氨酸和甲基丙二酸(MMA)在这些患者中的作用仍不清楚。我们希望通过对一名 cblC 缺乏症患者进行超过 6 年的随访,进一步阐明同型半胱氨酸和 MMA 水平作为血栓性微血管病(TMA)/aHUS 发病因素的作用。
一名 27 天大的西班牙裔女性因新生儿筛查中 C3-肉碱异常、喂养不良、活动减少和少尿而就诊。实验室结果显示血清同型半胱氨酸和 MMA 升高,基因检测显示 MMACHC 纯合致病性移码变异后,她被诊断为 cblC 缺乏症。该患者出现 aHUS 和急性肾损伤(AKI),经适当治疗后得到缓解。在超过 6 年的时间里,尽管同型半胱氨酸和 MMA 水平持续升高,但她的肾功能一直正常,没有血小板减少。
我们质疑同型半胱氨酸和 MMA 作为 cblC 缺乏症患者发生 aHUS/TMA 的原因,因为它们在随访期间持续升高,但并未导致 aHUS/TMA 或 AKI。其他代谢性疾病引起的高同型半胱氨酸血症和/或 MMA 并不会导致 aHUS/TMA 或 AKI。这表明其他肾毒性因素可能在 cblC 患者中引发 TMA。