Sathianathen Niranjan J, Pan Henry Y C, Furrer Marc, Thomas Benjamin, Dundee Philip, Corcoran Niall, Weight Christopher J, Konety Badrinath, Nair Rajesh, Lawrentschuk Nathan
Department of Surgery, University of Melbourne, Parkville, VIC, Australia.
Department of Urology, Royal Melbourne Hospital, Parkville, VIC, Australia.
Bladder Cancer. 2023 Sep 25;9(3):253-269. doi: 10.3233/BLC-220065. eCollection 2023.
The benefits of a robot-assisted radical cystectomy (RARC) compared to an open approach is still under debate. Initial data on RARC were from trials where urinary diversion was performed by an extracorporeal approach, which does not represent a completely minimally invasive procedure. There are now updated data for RARC with intracorporeal urinary diversion that add to the evidence profile of RARC.
To perform a systematic review and meta-analysis of the effectiveness of RARC compared with open radical cystectomy (ORC).
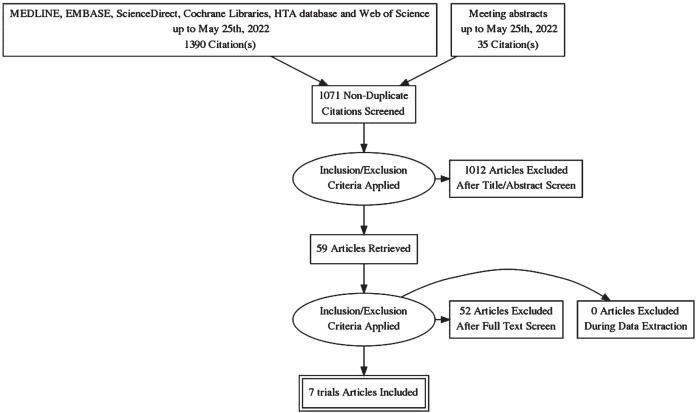
Multiple databases were searched up to May 2022. We included randomised trials in which patients underwent RARC and ORC. Oncological and safety outcomes were assessed.
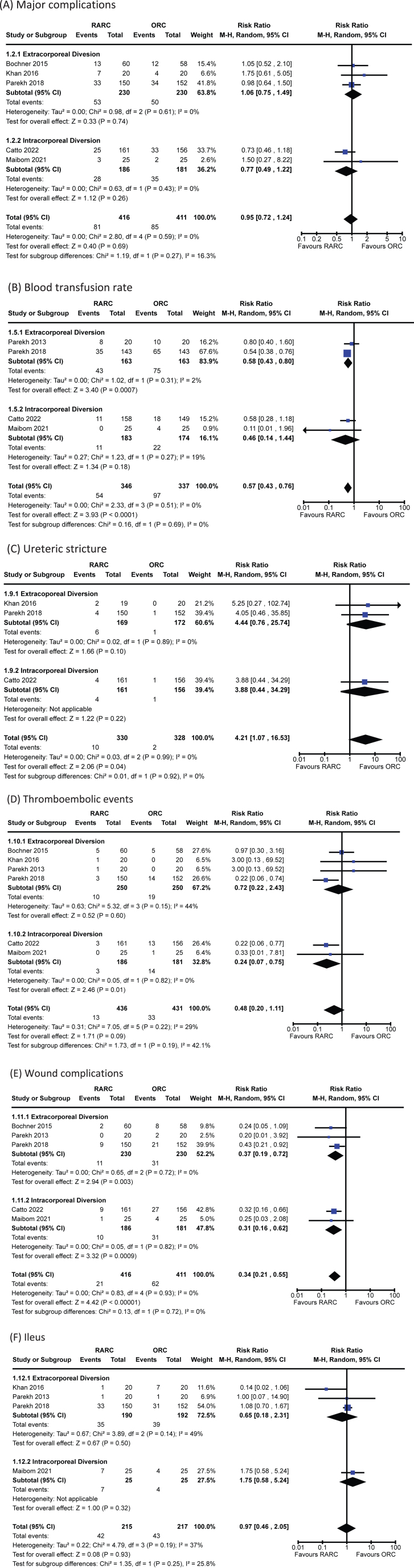
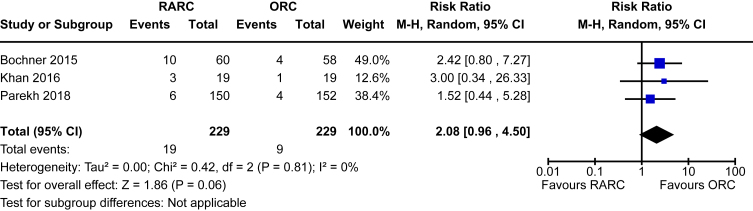
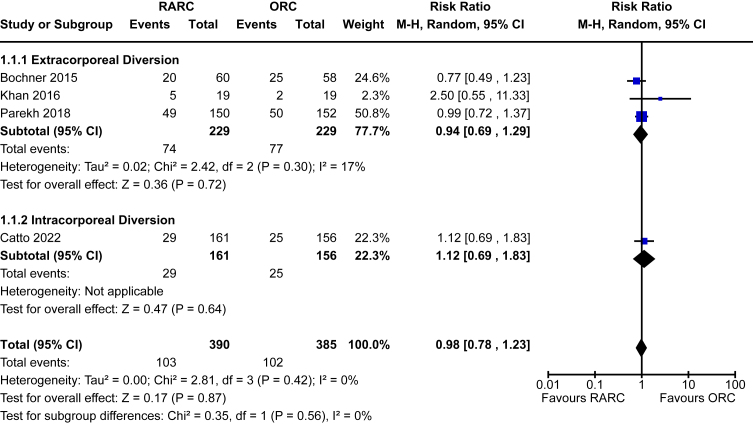
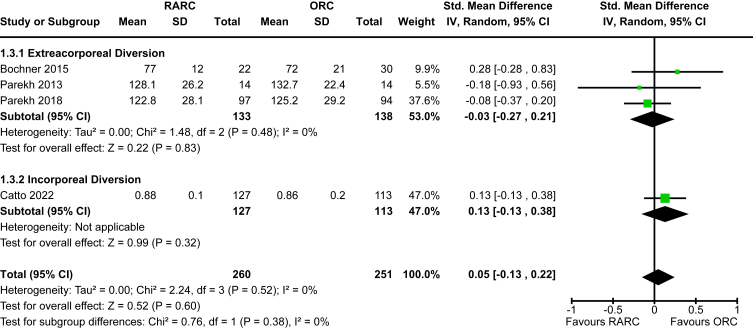
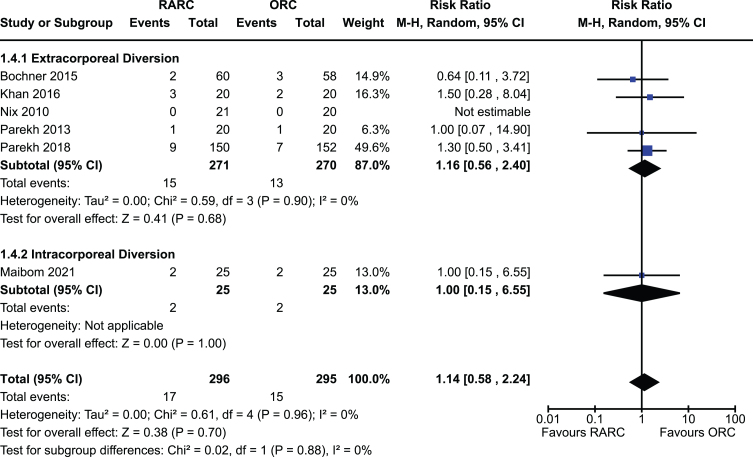
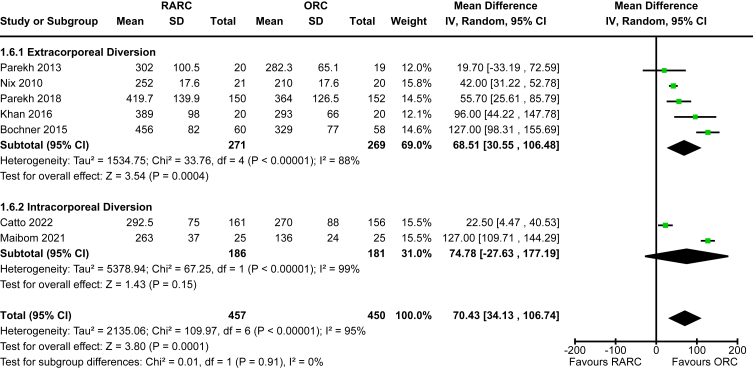
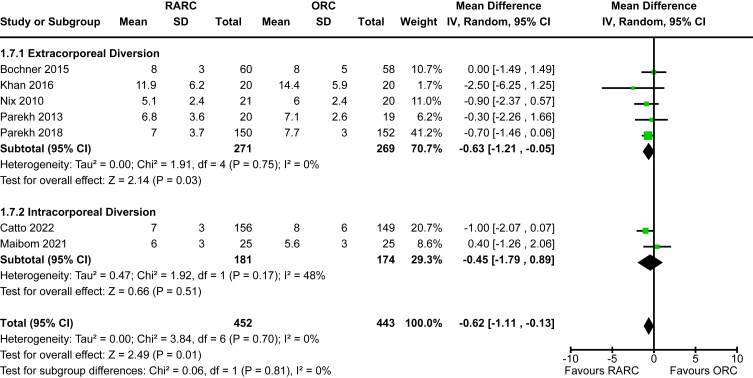
Seven trials of 907 participants were included. There were no differences seen in primary outcomes: disease progression [RR 0.98, 95% CI 0.78 to 1.23], major complications [RR 0.95, 95% CI 0.72 to 1.24] and quality of life [SMD 0.05, 95% CI -0.13 to 0.38]. RARC resulted in a decreased risk of perioperative blood transfusion [RR 0.57, 95% CI 0.43 to 0.76], wound complications [RR 0.34, 95% CI 0.21 to 0.55] and reduced length of hospital stay [MD -0.62 days, 95% CI -1.11 to -0.13]. However, there was an increased risk of developing a ureteric stricture [RR 4.21, 95% CI 1.07 to 16.53] in the RARC group and a prolonged operative time [MD 70.4 minutes, 95% CI 34.1 to 106.7]. The approach for urinary diversion did not impact outcomes.
RARC is an oncologically safe procedure compared to ORC and provides the benefits of a minimally invasive approach. There was an increased risk of developing a ureteric stricture in patients undergoing RARC that warrants further investigation. There was no difference in oncological outcomes between approaches.
与开放式手术相比,机器人辅助根治性膀胱切除术(RARC)的益处仍存在争议。RARC的初始数据来自于采用体外途径进行尿流改道的试验,这并非完全的微创手术。现在有了关于体内尿流改道的RARC的更新数据,增加了RARC的证据资料。
对RARC与开放式根治性膀胱切除术(ORC)的有效性进行系统评价和荟萃分析。
检索多个数据库至2022年5月。我们纳入了患者接受RARC和ORC的随机试验。评估肿瘤学和安全性结果。
纳入了7项试验,共907名参与者。主要结果未见差异:疾病进展[风险比(RR)0.98,95%置信区间(CI)0.78至1.23]、主要并发症[RR 0.95,95%CI 0.72至1.24]和生活质量[标准化均数差(SMD)0.05,95%CI -0.13至0.38]。RARC导致围手术期输血风险降低[RR 0.57,95%CI 0.43至0.76]、伤口并发症风险降低[RR 0.34,95%CI 0.21至0.55]以及住院时间缩短[平均差(MD)-0.62天,95%CI -1.11至-0.13]。然而,RARC组发生输尿管狭窄的风险增加[RR 4.21,95%CI 1.07至16.53],且手术时间延长[MD 70.4分钟,95%CI 34.1至106.7]。尿流改道方式不影响结果。
与ORC相比,RARC是一种肿瘤学上安全的手术,具有微创手术的益处。接受RARC的患者发生输尿管狭窄的风险增加,值得进一步研究。两种手术方式的肿瘤学结果无差异。