Department of Pulmonary & Critical Care Medicine.
Division of Pulmonary & Critical Care Medicine, Department of Internal Medicine.
Ann Am Thorac Soc. 2024 Nov;21(11):1560-1571. doi: 10.1513/AnnalsATS.202403-286OC.
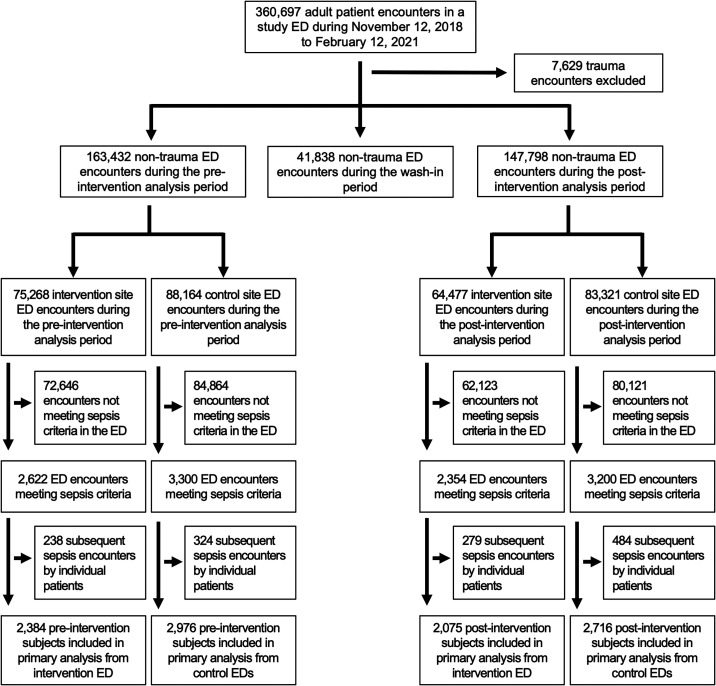
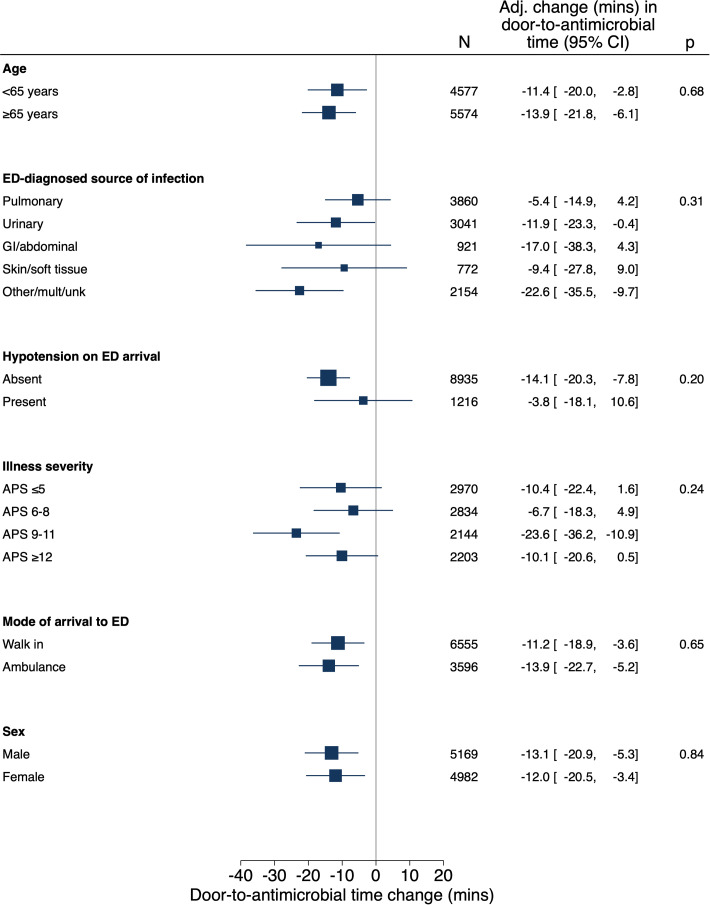
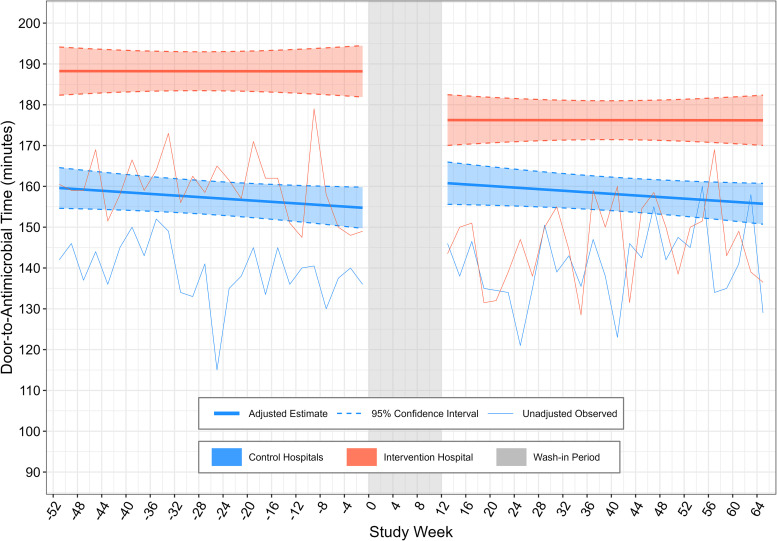
Sepsis care delivery-including the initiation of prompt, appropriate antimicrobials-remains suboptimal. This study was conducted to determine direct and off-target effects of emergency department (ED) sepsis care reorganization. This pragmatic pilot trial enrolled adult patients who presented from November 2019 to February 2021 to an ED in Utah before and after implementation of a multimodal, team-based "Code Sepsis" protocol. Patients who presented to two other EDs where usual care was continued served as contemporaneous control subjects. The primary outcome was door-to-antimicrobial time among patients meeting Sepsis-3 criteria before ED departure. Secondary and safety outcomes included all-cause 30-day mortality, antimicrobial utilization and overtreatment, and antimicrobial-associated adverse events. Multivariable regression analyses used difference-in-differences methods to account for trends in outcomes unrelated to the studied intervention. Code Sepsis protocol activation ( = 307) exhibited 8.5% sensitivity and 66% positive predictive value for patients meeting sepsis criteria before ED departure. Among 10,151 patients who met sepsis criteria during the study, adjusted difference-in-differences analysis demonstrated a 13-minute (95% confidence interval = 7-19) decrease in door-to-antimicrobial time associated with Code Sepsis implementation ( < 0.001). Mortality and clinical safety outcomes were unchanged, but Code Sepsis implementation was associated with increased false-positive presumptive infection diagnoses among patients who met sepsis criteria in the ED and increased antimicrobial utilization. Implementation of a team-based protocol for rapid sepsis evaluation and treatment during the coronavirus disease (COVID-19) pandemic's first year was associated with decreased ED door-to-antimicrobial time but also increased antimicrobial utilization. Measurement of both patient-centered and off-target effects of sepsis care improvement interventions is essential to comprehensive assessment of their value. Clinical trial registered with www.clinicaltrials.gov (NCT04148989).
脓毒症的治疗护理(包括及时、合理使用抗生素)仍不理想。本研究旨在评估急诊(ED)脓毒症治疗护理重组的直接和非靶向影响。这是一项实用的试点试验,纳入了 2019 年 11 月至 2021 年 2 月间,在犹他州一家 ED 就诊且符合 Sepsis-3 标准的成年患者,这些患者在 ED 接受了多模式、团队合作的“Code Sepsis”方案治疗后,与另外两家 ED 就诊且继续采用常规治疗的患者作为同期对照。主要结局为 ED 离开前符合 Sepsis-3 标准的患者的门到抗生素时间。次要结局和安全性结局包括 30 天全因死亡率、抗生素使用和过度治疗,以及抗生素相关不良事件。多变量回归分析采用差异中的差异方法,以解释与研究干预无关的结局趋势。Code Sepsis 方案的启动( = 307)对 ED 离开前符合脓毒症标准的患者具有 8.5%的敏感性和 66%的阳性预测值。在研究期间符合脓毒症标准的 10151 名患者中,调整后的差异中的差异分析表明,与 Code Sepsis 实施相关,门到抗生素时间减少了 13 分钟(95%置信区间 7-19)( < 0.001)。死亡率和临床安全性结局没有变化,但 Code Sepsis 的实施与 ED 中符合脓毒症标准的患者中假阳性推定感染诊断的增加以及抗生素使用的增加有关。在 COVID-19 大流行的第一年,实施基于团队的快速脓毒症评估和治疗方案与 ED 门到抗生素时间的缩短有关,但也与抗生素使用的增加有关。对脓毒症治疗干预的以患者为中心的和非靶向影响进行测量,对于全面评估其价值至关重要。该研究在 www.clinicaltrials.gov 注册(NCT04148989)。