Department of Thoracic Surgery, Guangdong Provincial People's Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, People's Republic of China.
Department of Radiology, Jiangxi Cancer Hospital, Nanchang, People's Republic of China.
J Immunother Cancer. 2023 Oct;11(10). doi: 10.1136/jitc-2023-007369.
The predictive efficacy of current biomarker of immune checkpoint inhibitors (ICIs) is not sufficient. This study investigated the causality between radiomic biomarkers and immunotherapy response status in patients with stage IB-IV non-small cell lung cancer (NSCLC), including its biological context for ICIs treatment response prediction.
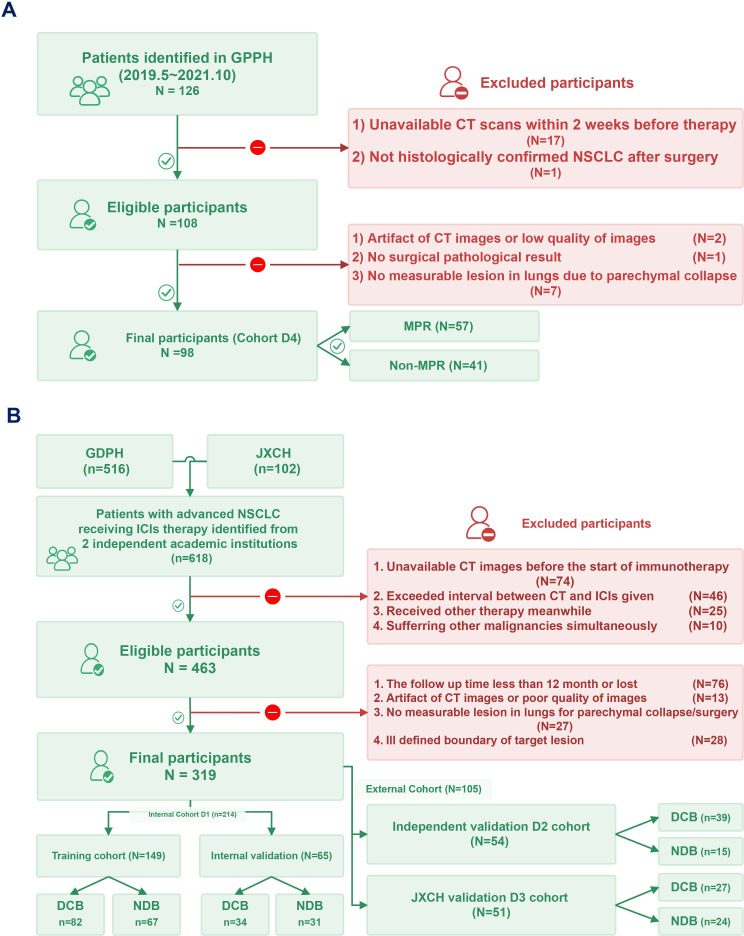
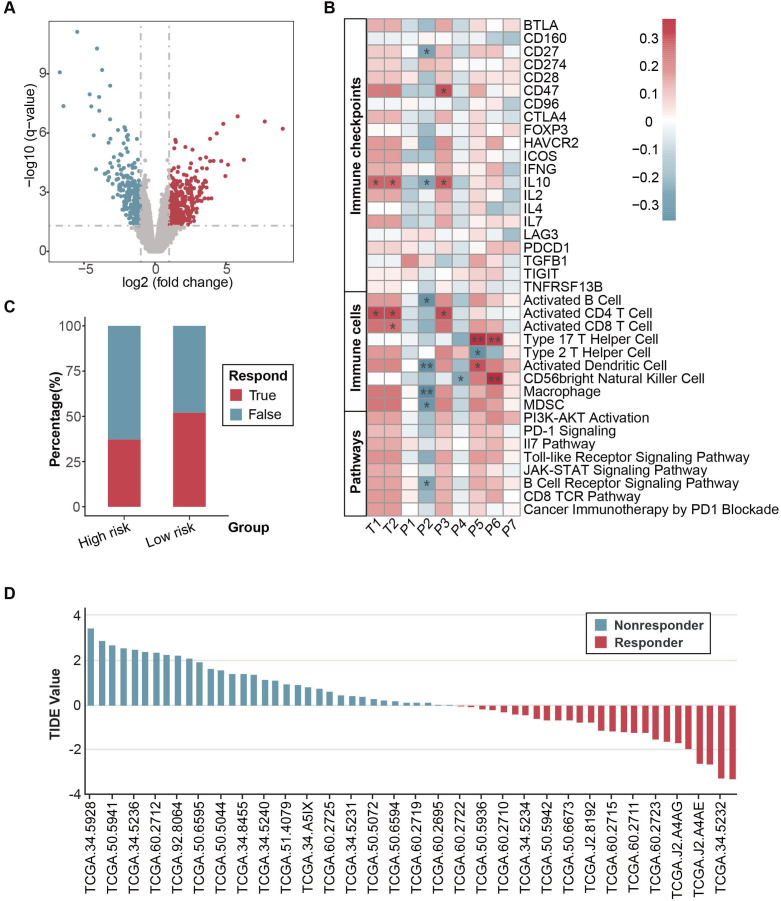
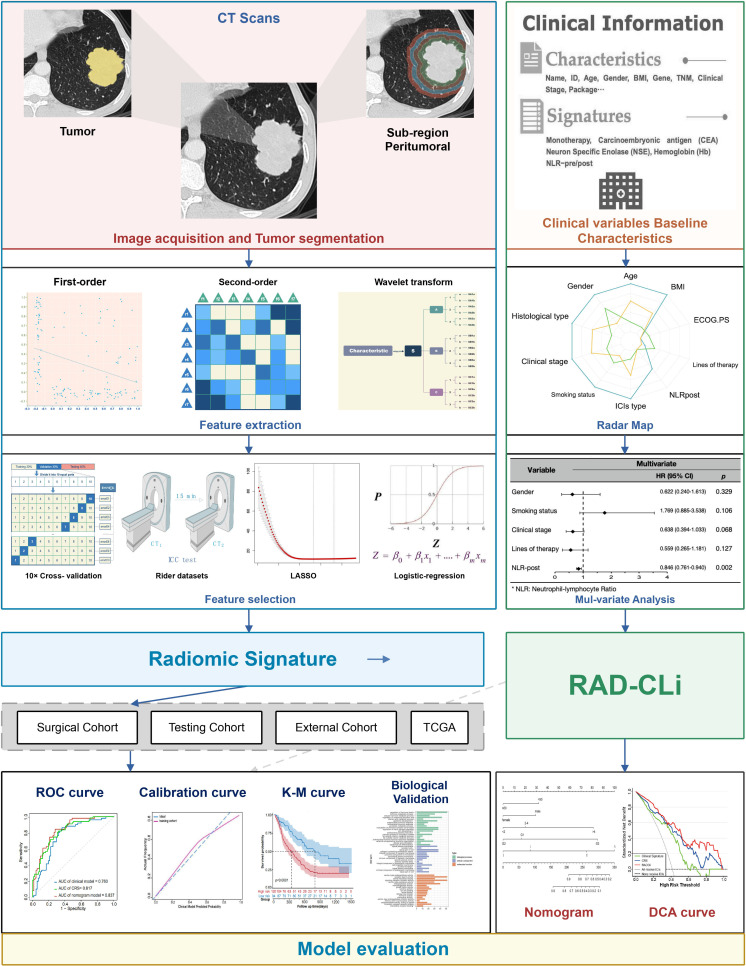
CT images from 319 patients with pretreatment NSCLC receiving immunotherapy between January 2015 and November 2021 were retrospectively collected and composed a discovery (n=214), independent validation (n=54), and external test cohort (n=51). A set of 851 features was extracted from tumorous and peritumoral volumes of interest (VOIs). The reference standard is the durable clinical benefit (DCB, sustained disease control for more than 6 months assessed via radiological evaluation). The predictive value of combined radiomic signature (CRS) for pathological response was subsequently assessed in another cohort of 98 patients with resectable NSCLC receiving ICIs preoperatively. The association between radiomic features and tumor immune landscape on the online data set (n=60) was also examined. A model combining clinical predictor and radiomic signatures was constructed to improve performance further.
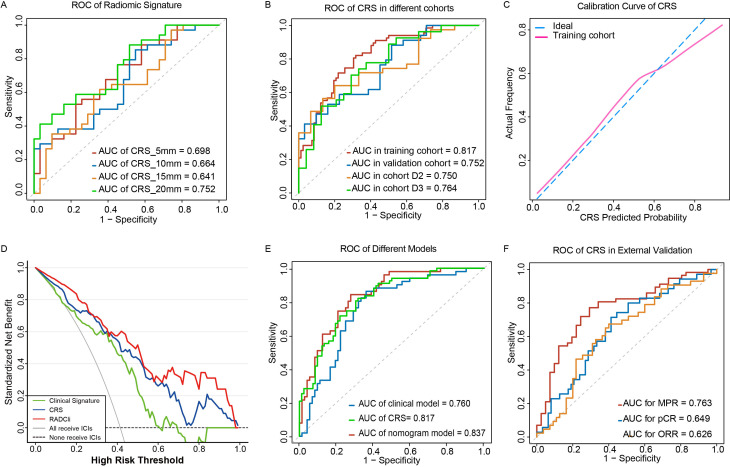
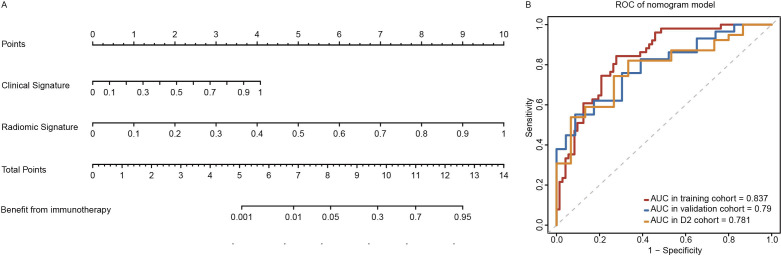
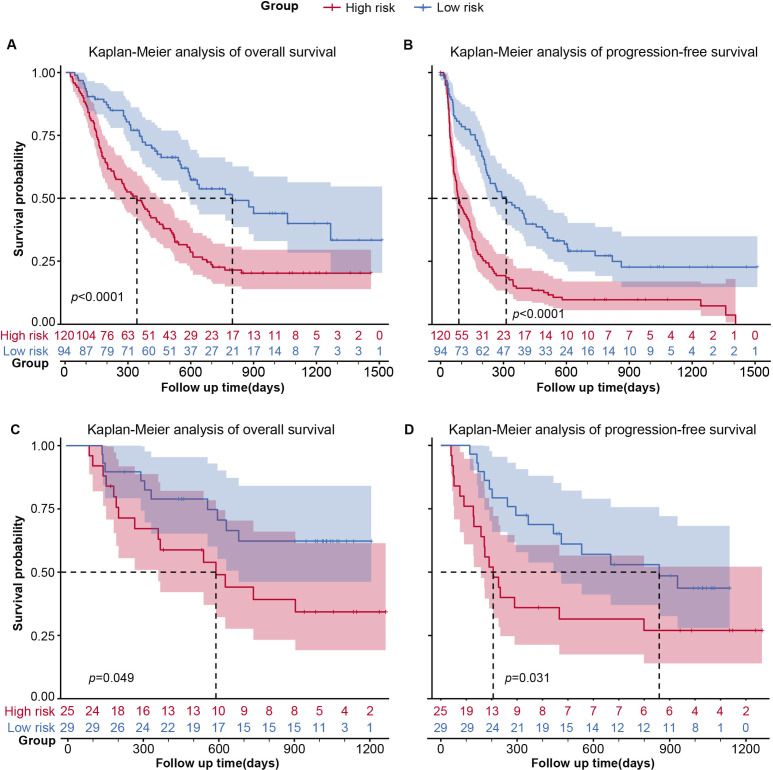
CRS discriminated DCB and non-DCB patients well in the training and validation cohorts with an area under the curve (AUC) of 0.82, 95% CI: 0.75 to 0.88, and 0.75, 95% CI: 0.64 to 0.87, respectively. In this study, the predictive value of CRS was better than programmed cell death ligand-1 (PD-L1) expression (AUC of PD-L1 subset: 0.59, 95% CI: 0.50 to 0.69) or clinical model (AUC: 0.66, 95% CI: 0.51 to 0.81). After combining the clinical signature with CRS, the predictive performance improved further with an AUC of 0.837, 0.790 and 0.781 in training, validation and D2 cohorts, respectively. When predicting pathological response, CRS divided patients into a major pathological response (MPR) and non-MPR group (AUC: 0.76, 95% CI: 0.67 to 0.81). Moreover, CRS showed a promising stratification ability on overall survival (HR: 0.49, 95% CI: 0.27 to 0.89; p=0.020) and progression-free survival (HR: 0.43, 95% CI: 0.26 to 0.74; p=0.002).
By analyzing both tumorous and peritumoral regions of CT images in a radiomic strategy, we developed a non-invasive biomarker for distinguishing responders of ICIs therapy and stratifying their survival outcome efficiently, which may support the clinical decisions on the use of ICIs in advanced as well as patients with resectable NSCLC.
目前免疫检查点抑制剂(ICI)的生物标志物预测疗效并不充分。本研究旨在探讨影像学生物标志物与接受免疫治疗的 I 期至 IV 期非小细胞肺癌(NSCLC)患者治疗反应状态之间的因果关系,包括其在预测ICI 治疗反应方面的生物学背景。
回顾性收集了 2015 年 1 月至 2021 年 11 月期间接受免疫治疗的 319 例 NSCLC 患者的预处理 CT 图像,并将其组成发现队列(n=214)、独立验证队列(n=54)和外部测试队列(n=51)。从肿瘤和肿瘤周围感兴趣区(VOI)中提取了一组 851 个特征。参考标准为持久临床获益(DCB,通过影像学评估持续疾病控制超过 6 个月)。随后,在另一组 98 例接受 ICI 术前治疗的可切除 NSCLC 患者中评估了联合放射组学特征(CRS)对病理反应的预测价值。还检查了在线数据集(n=60)上放射组学特征与肿瘤免疫景观之间的关联。构建了一个结合临床预测因子和放射组学特征的模型,以进一步提高性能。
CRS 在训练和验证队列中很好地区分了 DCB 和非 DCB 患者,曲线下面积(AUC)分别为 0.82(95%CI:0.75 至 0.88)和 0.75(95%CI:0.64 至 0.87)。在这项研究中,CRS 的预测价值优于程序性细胞死亡配体-1(PD-L1)表达(PD-L1 亚组 AUC:0.59,95%CI:0.50 至 0.69)或临床模型(AUC:0.66,95%CI:0.51 至 0.81)。在结合临床特征与 CRS 后,预测性能进一步提高,在训练、验证和 D2 队列中的 AUC 分别为 0.837、0.790 和 0.781。当预测病理反应时,CRS 将患者分为主要病理反应(MPR)和非 MPR 组(AUC:0.76,95%CI:0.67 至 0.81)。此外,CRS 显示出在总生存期(HR:0.49,95%CI:0.27 至 0.89;p=0.020)和无进展生存期(HR:0.43,95%CI:0.26 至 0.74;p=0.002)方面具有有前景的分层能力。
通过分析 CT 图像的肿瘤和肿瘤周围区域的放射组学特征,我们开发了一种非侵入性生物标志物,用于区分 ICI 治疗反应者,并有效地分层其生存结果,这可能支持在晚期和可切除 NSCLC 患者中使用 ICI 的临床决策。