Ahmed Kedir Y, Thapa Subash, Hassen Tahir A, Tegegne Teketo Kassaw, Dadi Abel F, Odo Daniel Bogale, Bizuayehu Habtamu Mellie, Shifti Desalegn Markos, Belachew Sewunet Admasu, Kibret Getiye Dejenu, Ketema Daniel Bekele, Kassa Zemenu Yohannes, Amsalu Erkihun, Bore Meless G, Seid Abdulbasit, Mesfin Yonatan M, Kibret Kelemu Tilahun, Huda M Mamun, Mahmood Shakeel, Anyasodor Anayochukwu E, Ross Allen G
Rural Health Research Institute, Charles Sturt University, Orange, NSW 2800, Australia.
Center for Women's Health Research, College of Health, Medicine and Wellbeing, The University of Newcastle, NSW, Australia.
EClinicalMedicine. 2024 Jun 20;73:102682. doi: 10.1016/j.eclinm.2024.102682. eCollection 2024 Jul.
Sub-Saharan Africa (SSA) has the highest burden of neonatal mortality in the world. Identifying the most critical modifiable risk factors is imperative for reducing neonatal mortality rates. This study is the first to calculate population-attributable fractions (PAFs) for modifiable risk factors of neonatal mortality in SSA.
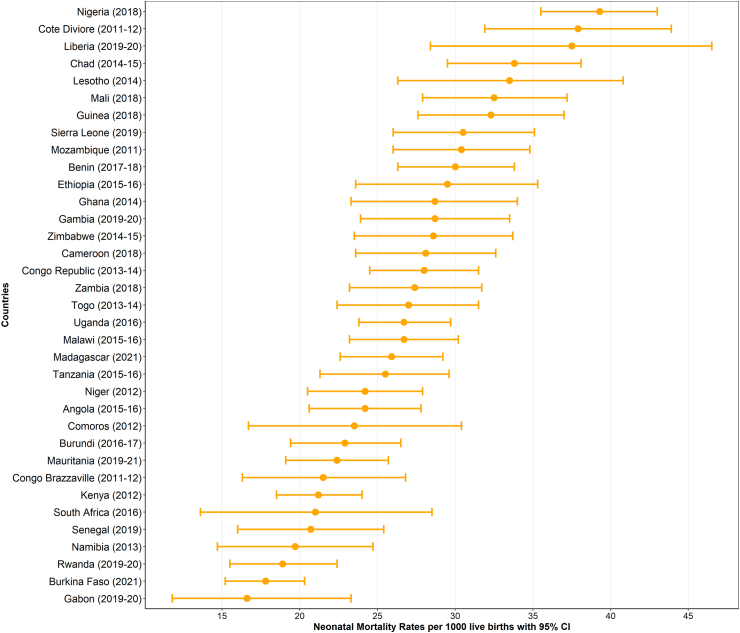
We analysed the most recent Demographic and Health Surveys data sets from 35 SSA countries conducted between 2010 and 2022. Generalized linear latent and mixed models were used to estimate odds ratios (ORs) along with 95% confidence intervals (CIs). PAFs adjusted for communality were calculated using ORs and prevalence estimates for key modifiable risk factors. Subregional analyses were conducted to examine variations in modifiable risk factors for neonatal mortality across Central, Eastern, Southern, and Western SSA regions.
In this study, we included 255,891 live births in the five years before the survey. The highest PAFs of neonatal mortality among singleton children were attributed to delayed initiation of breastfeeding (>1 h after birth: PAF = 23.88%; 95% CI: 15.91, 24.86), uncleaned cooking fuel (PAF = 5.27%; 95% CI: 1.41, 8.73), mother's lacking formal education (PAF = 4.34%; 95% CI: 1.15, 6.31), mother's lacking tetanus vaccination (PAF = 3.54%; 95% CI: 1.55, 4.92), and infrequent antenatal care (ANC) visits (PAF = 2.45; 95% CI: 0.76, 3.63). Together, these five modifiable risk factors were associated with 39.49% (95% CI: 21.13, 48.44) of neonatal deaths among singleton children in SSA. Our subregional analyses revealed some variations in modifiable risk factors for neonatal mortality. Notably, delayed initiation of breastfeeding consistently contributed to the highest PAFs of neonatal mortality across all four regions of SSA: Central, Eastern, Southern, and Western SSA.
The PAF estimates in the present study indicate that a considerable proportion of neonatal deaths in SSA are preventable. We identified five modifiable risk factors that accounted for approximately 40% of neonatal deaths in SSA. The findings have policy implications.
None.
撒哈拉以南非洲地区(SSA)是全球新生儿死亡率最高的地区。确定最关键的可改变风险因素对于降低新生儿死亡率至关重要。本研究首次计算了SSA地区新生儿死亡率可改变风险因素的人群归因分数(PAF)。
我们分析了2010年至2022年期间35个SSA国家的最新人口与健康调查数据集。使用广义线性潜在和混合模型估计比值比(OR)以及95%置信区间(CI)。使用OR和关键可改变风险因素的患病率估计值计算经共性调整的PAF。进行了次区域分析,以研究SSA中部、东部、南部和西部各地区新生儿死亡率可改变风险因素的差异。
在本研究中,我们纳入了调查前五年内的255,891例活产。单胎新生儿中,新生儿死亡率的最高PAF归因于母乳喂养开始延迟(出生后>1小时:PAF = 23.88%;95% CI:15.91,24.86)、未清洁的烹饪燃料(PAF = 5.27%;95% CI:1.41,8.73)、母亲缺乏正规教育(PAF = 4.34%;95% CI:1.15,6.31)、母亲未接种破伤风疫苗(PAF = 3.54%;95% CI:1.55,4.92)以及产前检查(ANC)次数少(PAF = 2.45;95% CI:0.76,3.63)。这五个可改变风险因素共同导致了SSA地区单胎新生儿中39.49%(95% CI:21.13,48.44)的新生儿死亡。我们的次区域分析揭示了新生儿死亡率可改变风险因素的一些差异。值得注意的是,母乳喂养开始延迟在SSA所有四个地区(中部、东部、南部和西部)始终导致最高的新生儿死亡率PAF。
本研究中的PAF估计表明,SSA地区相当一部分新生儿死亡是可预防的。我们确定了五个可改变风险因素,它们占SSA地区新生儿死亡的约40%。这些发现具有政策意义。
无。