Mkumbo Elibariki Godfrey, Willows Tamara Mulenga, Odongo Onyango Onesmus, Khalid Karima, Maiba John, Schell Carl Otto, Oliwa Jacquie, McKnight Jacob, Baker Tim
The Health Systems, Impact Evaluation and Policy Department, Ifakara Health Institute, Dar Es Salaam, Tanzania.
Health Systems Collaborative, University of Oxford/ Wolfson Institute of Population Health, Queen Mary's University London, London, UK.
BMC Health Serv Res. 2024 Jul 17;24(1):821. doi: 10.1186/s12913-024-11254-y.
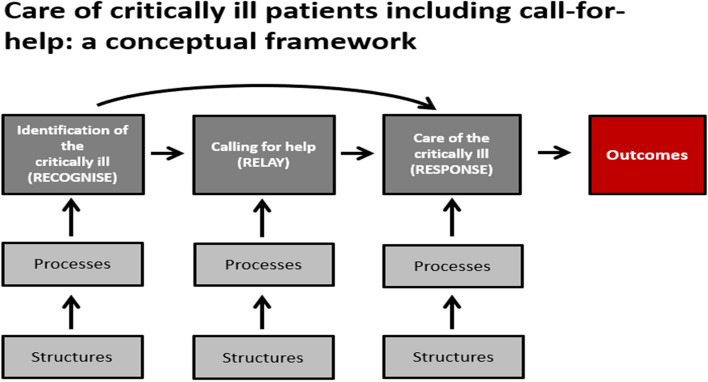
When caring for critically ill patients, health workers often need to 'call-for-help' to get assistance from colleagues in the hospital. Systems are required to facilitate calling-for-help and enable the timely provision of care for critically ill patients. Evidence around calling-for-help systems is mostly from high income countries and the state of calling-for-help in hospitals in Tanzania and Kenya has not been formally studied. This study aims to describe health workers' experiences about calling-for-help when taking care of critically ill patients in hospitals in Tanzania and Kenya.
Ten hospitals across Kenya and Tanzania were visited and in-depth interviews conducted with 30 health workers who had experience of caring for critically ill patients. The interviews were transcribed, translated and the data thematically analyzed.
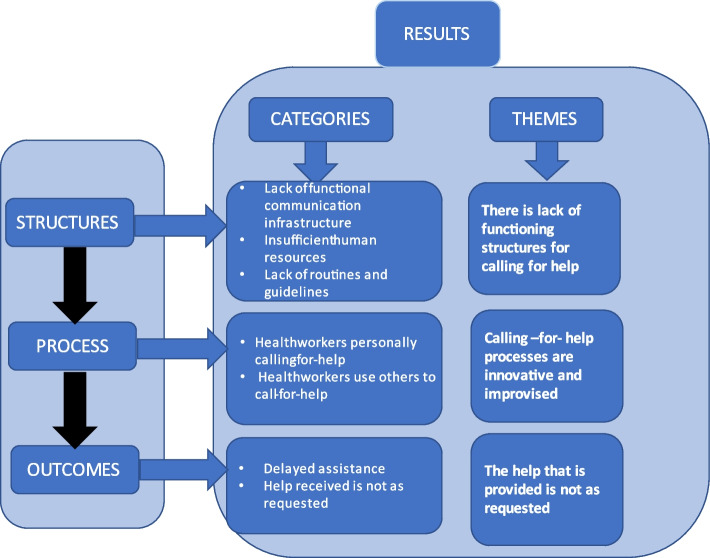
The study identified three thematic areas concerning the systems for calling-for-help when taking care of critically ill patients: 1) Calling-for-help structures: there is lack of functioning structures for calling-for-help; 2) Calling-for-help processes: the calling-for-help processes are innovative and improvised; and 3) Calling-for-help outcomes: the help that is provided is not as requested.
Calling-for-help when taking care of a critically ill patient is a necessary life-saving part of care, but health workers in Tanzanian and Kenyan hospitals experience a range of significant challenges. Hospitals lack functioning structures, processes for calling-for-help are improvised and help that is provided is not as requested. These challenges likely cause delays and decrease the quality of care, potentially resulting in unnecessary mortality and morbidity.
在照顾重症患者时,医护人员经常需要“呼救”以获得医院同事的帮助。需要有相应系统来便利呼救,并确保能及时为重症患者提供护理。关于呼救系统的证据大多来自高收入国家,而坦桑尼亚和肯尼亚医院的呼救状况尚未得到正式研究。本研究旨在描述坦桑尼亚和肯尼亚医院的医护人员在照顾重症患者时的呼救经历。
走访了肯尼亚和坦桑尼亚的10家医院,并对30名有照顾重症患者经验的医护人员进行了深入访谈。对访谈内容进行了转录、翻译,并对数据进行了主题分析。
该研究确定了照顾重症患者时呼救系统的三个主题领域:1)呼救结构:缺乏有效的呼救结构;2)呼救流程:呼救流程是创新且临时拼凑的;3)呼救结果:所提供的帮助并非如所请求的那样。
照顾重症患者时呼救是护理中必要的救命环节,但坦桑尼亚和肯尼亚医院的医护人员面临一系列重大挑战。医院缺乏有效的结构,呼救流程是临时拼凑的,所提供的帮助并非如所请求的那样。这些挑战可能导致延误并降低护理质量, potentially resulting in unnecessary mortality and morbidity.(此处原英文有误,正确翻译为“可能导致不必要的死亡和发病”)