Ack Sophie E, Dolmans Rianne G F, Foreman Brandon, Manley Geoffrey T, Rosenthal Eric S, Zabihi Morteza
Department of Neurology, Massachusetts General Hospital, Harvard Medical School, Boston, MA.
Department of Neurosurgery, Leiden University Medical Center, Leiden, The Netherlands.
Crit Care Explor. 2024 Jul 16;6(7):e1118. doi: 10.1097/CCE.0000000000001118. eCollection 2024 Jul 1.
Treatment for intracranial pressure (ICP) has been increasingly informed by machine learning (ML)-derived ICP waveform characteristics. There are gaps, however, in understanding how ICP monitor type may bias waveform characteristics used for these predictive tools since differences between external ventricular drain (EVD) and intraparenchymal monitor (IPM)-derived waveforms have not been well accounted for.
We sought to develop a proof-of-concept ML model differentiating ICP waveforms originating from an EVD or IPM.
DESIGN, SETTING, AND PARTICIPANTS: We examined raw ICP waveform data from the ICU physiology cohort within the prospective Transforming Research and Clinical Knowledge in Traumatic Brain Injury multicenter study.
Nested patient-wise five-fold cross-validation and group analysis with bagged decision trees (BDT) and linear discriminant analysis were used for feature selection and fair evaluation. Nine patients were kept as unseen hold-outs for further evaluation.
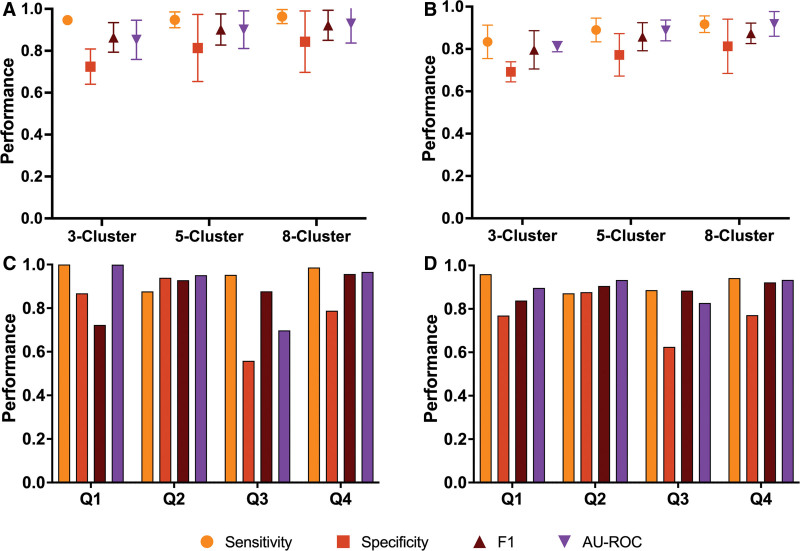
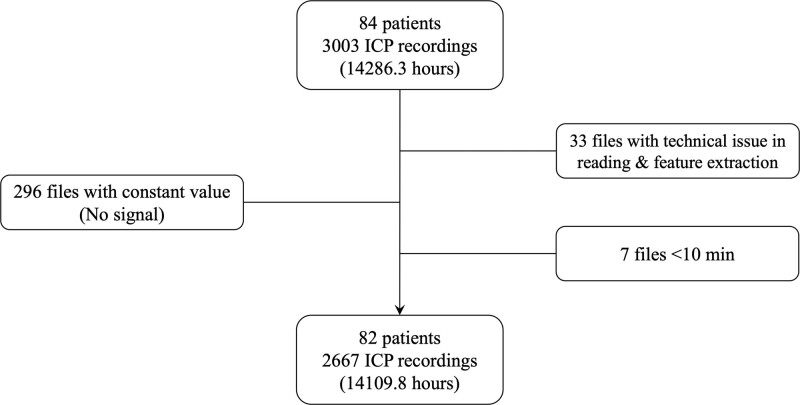
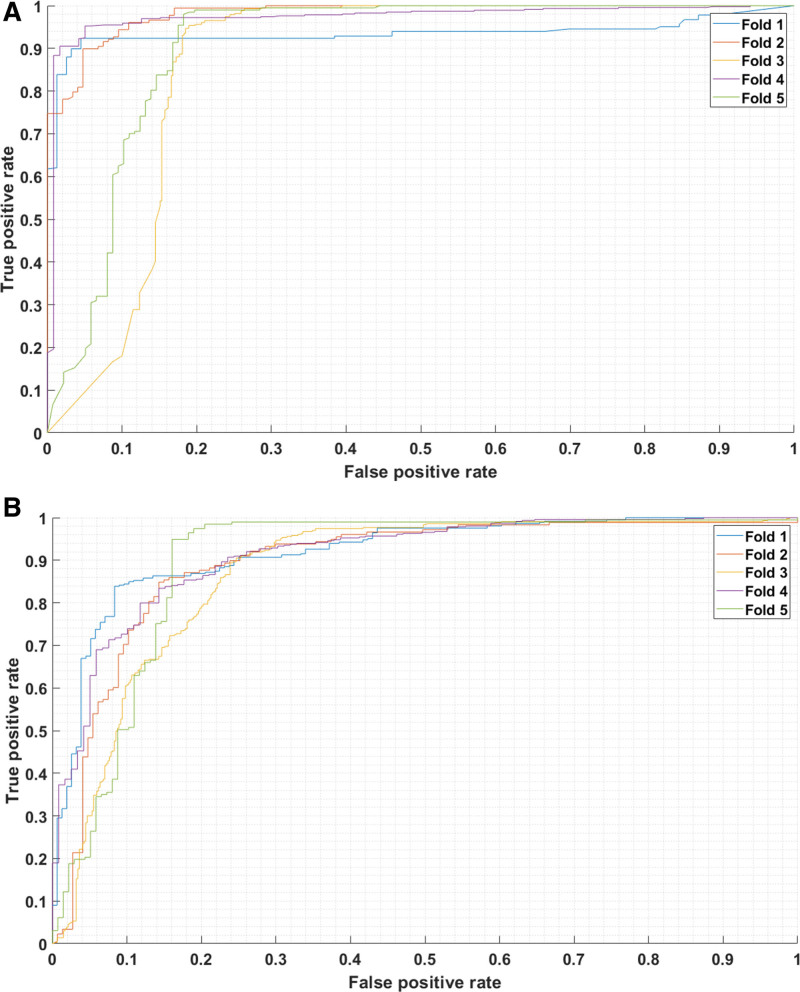
ICP waveform data totaling 14,110 hours were included from 82 patients (EVD, 47; IPM, 26; both, 9). Mean age, Glasgow Coma Scale (GCS) total, and GCS motor score upon admission, as well as the presence and amount of midline shift, were similar between groups. The model mean area under the receiver operating characteristic curve (AU-ROC) exceeded 0.874 across all folds. In additional rigorous cluster-based subgroup analysis, targeted at testing the resilience of models to cross-validation with smaller subsets constructed to develop models in one confounder set and test them in another subset, AU-ROC exceeded 0.811. In a similar analysis using propensity score-based rather than cluster-based subgroup analysis, the mean AU-ROC exceeded 0.827. Of 842 extracted ICP features, 62 were invariant within every analysis, representing the most accurate and robust differences between ICP monitor types. For the nine patient hold-outs, an AU-ROC of 0.826 was obtained using BDT.
The developed proof-of-concept ML model identified differences in EVD- and IPM-derived ICP signals, which can provide missing contextual data for large-scale retrospective datasets, prevent bias in computational models that ingest ICP data indiscriminately, and control for confounding using our model's output as a propensity score by to adjust for the monitoring method that was clinically indicated. Furthermore, the invariant features may be leveraged as ICP features for anomaly detection.
机器学习(ML)得出的颅内压(ICP)波形特征越来越多地为ICP治疗提供依据。然而,在理解ICP监测类型如何可能使这些预测工具所使用的波形特征产生偏差方面存在差距,因为脑室外引流管(EVD)和脑实质内监测器(IPM)得出的波形之间的差异尚未得到充分考虑。
我们试图开发一个概念验证性ML模型,以区分源自EVD或IPM的ICP波形。
设计、设置和参与者:我们检查了前瞻性创伤性脑损伤转化研究与临床知识多中心研究中ICU生理学队列的原始ICP波形数据。
采用嵌套的患者层面五折交叉验证以及使用袋装决策树(BDT)和线性判别分析的组分析进行特征选择和公平评估。九名患者被留作未见过的保留样本用于进一步评估。
纳入了82名患者的总计14110小时的ICP波形数据(EVD组47例;IPM组26例;两组均有的9例)。各组之间的平均年龄、入院时格拉斯哥昏迷量表(GCS)总分和GCS运动评分,以及中线移位的存在情况和程度相似。所有折次的模型平均受试者工作特征曲线下面积(AU-ROC)均超过0.874。在另外一项基于严格聚类的亚组分析中,旨在测试模型对交叉验证的弹性,该交叉验证使用在一个混杂因素集构建模型并在另一个子集中进行测试的较小子集,AU-ROC超过0.811。在一项使用基于倾向评分而非基于聚类的亚组分析的类似分析中,平均AU-ROC超过0.827。在提取的842个ICP特征中,62个在每次分析中都是不变的,代表了ICP监测类型之间最准确和最稳健的差异。对于九名保留样本患者,使用BDT获得的AU-ROC为0.826。
所开发的概念验证性ML模型识别出了EVD和IPM得出的ICP信号中的差异,这可为大规模回顾性数据集提供缺失的背景数据,防止不加区分地摄取ICP数据的计算模型出现偏差,并通过将我们模型的输出用作倾向评分来控制混杂因素,以调整临床指示的监测方法。此外,这些不变特征可作为ICP特征用于异常检测。