World-Class Research Center «Digital Biodesign and Personalized Healthcare», I.M. Sechenov First Moscow State Medical University (Sechenov University), 119991 Moscow, Russia.
Curr Cardiol Rev. 2024;20(6):e190724232038. doi: 10.2174/011573403X302934240715113647.
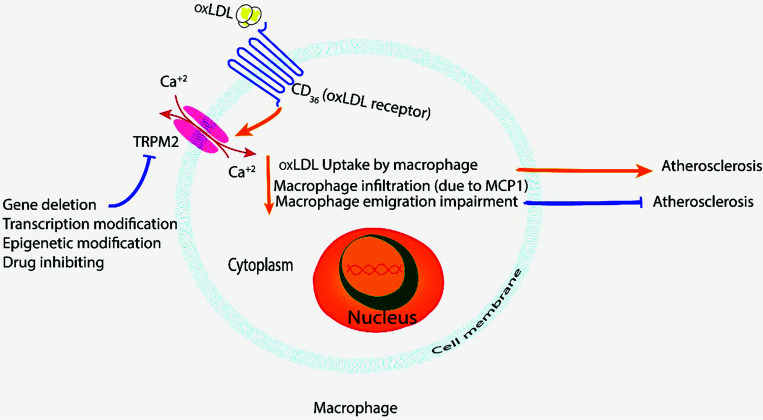
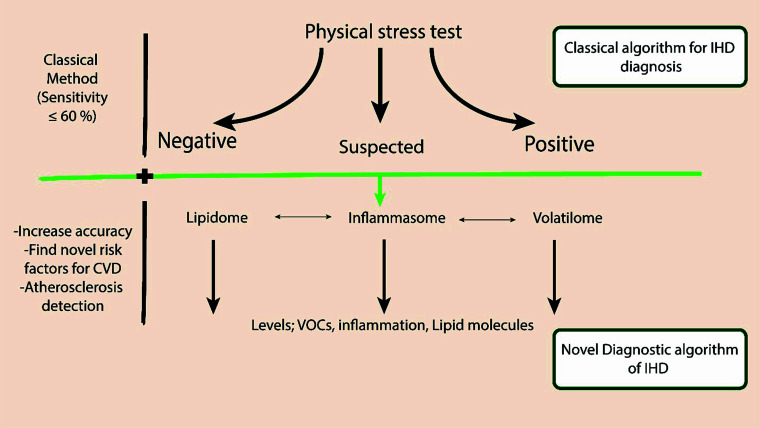
Ischemic heart disease (IHD) is a pathology of global interest because it is widespread and has high morbidity and mortality. IHD pathophysiology involves local and systemic changes, including lipidomic, proteomic, and inflammasome changes in serum plasma. The modulation in these metabolites is viable in the pre-IHD, during the IHD period, and after management of IHD in all forms, including lifestyle changes and pharmacological and surgical interventions. Therefore, these biochemical markers (metabolite changes; lipidome, inflammasome, proteome) can be used for early prevention, treatment strategy, assessment of the patient's response to the treatment, diagnosis, and determination of prognosis. Lipidomic changes are associated with the severity of inflammation and disorder in the lipidome component, and correlation is related to disturbance of inflammasome components. Main inflammasome biomarkers that are associated with coronary artery disease progression include IL-1β, Nucleotide-binding oligomerization domain- like receptor family pyrin domain containing 3 (NLRP3), and caspase-1. Meanwhile, the main lipidome biomarkers related to coronary artery disease development involve plasmalogen lipids, lysophosphatidylethanolamine (LPE), and phosphatidylethanolamine (PE). The hypothesis of this paper is that the changes in the volatile organic compounds associated with inflammasome and lipidome changes in patients with coronary artery disease are various and depend on the severity and risk factor for death from cardiovascular disease in the time span of 10 years. In this paper, we explore the potential origin and pathway in which the lipidome and or inflammasome molecules could be excreted in the exhaled air in the form of volatile organic compounds (VOCs).
缺血性心脏病(IHD)是一种具有全球意义的病理学,因为它广泛存在且发病率和死亡率都很高。IHD 的病理生理学涉及局部和全身变化,包括血清血浆中的脂质组学、蛋白质组学和炎症小体变化。这些代谢物的调节在 IHD 前、IHD 期间以及 IHD 管理后(包括生活方式改变和药物及手术干预)的所有形式中都是可行的。因此,这些生化标志物(代谢物变化;脂质组学、炎症小体、蛋白质组学)可用于早期预防、治疗策略、评估患者对治疗的反应、诊断和预后判断。脂质组学变化与炎症的严重程度和脂质组学成分的紊乱有关,相关性与炎症小体成分的紊乱有关。与冠状动脉疾病进展相关的主要炎症小体生物标志物包括白细胞介素-1β(IL-1β)、核苷酸结合寡聚结构域样受体家族含pyrin 结构域 3(NLRP3)和半胱天冬酶-1。同时,与冠状动脉疾病发展相关的主要脂质组学生物标志物涉及类质体脂质、溶血磷脂酰乙醇胺(LPE)和磷脂酰乙醇胺(PE)。本文的假设是,与冠心病患者炎症小体和脂质组学变化相关的挥发性有机化合物的变化是多种多样的,并且取决于 10 年内心血管疾病死亡的严重程度和危险因素。在本文中,我们探讨了脂质组学和/或炎症小体分子以挥发性有机化合物(VOC)形式在呼出空气中排泄的潜在起源和途径。