Division of Biostatistics, Department of Population Health, New York University Langone Medical Center, New York.
Department of Medicine, New York University Langone Medical Center, New York.
JAMA Netw Open. 2024 Jul 1;7(7):e2424519. doi: 10.1001/jamanetworkopen.2024.24519.
While the association between cross-sectional measures of social isolation and adverse health outcomes is well established, less is known about the association between changes in social isolation and health outcomes.
To assess changes of social isolation and mortality, physical function, cognitive function, cardiovascular disease (CVD), and stroke.
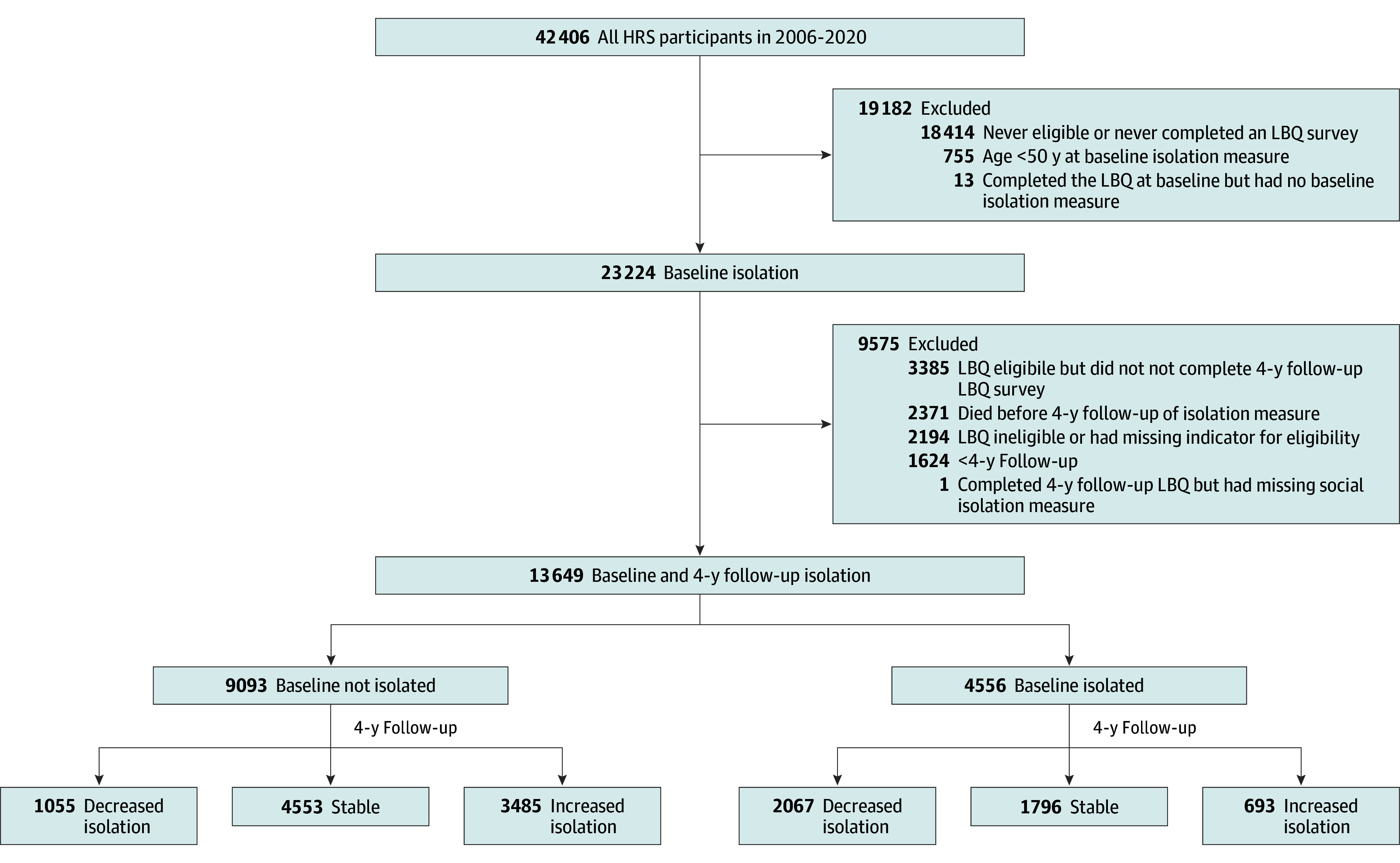
DESIGN, SETTING, AND PARTICIPANTS: In a cohort design, social isolation changes in 4 years and subsequent risk of mortality and other outcomes were assessed using the 13 649 eligible Health and Retirement Study (HRS) respondents from the 2006 to 2020 waves. Data were analyzed from October 11, 2023, to April 26, 2024.
The main exposure was the change in social isolation measured by the Steptoe 5-item Social Isolation Index from the initial assessment to a second assessment conducted 4 years later. Participants were classified into decreased isolation, stable, or increased isolation groups, stratified by their baseline isolation status.
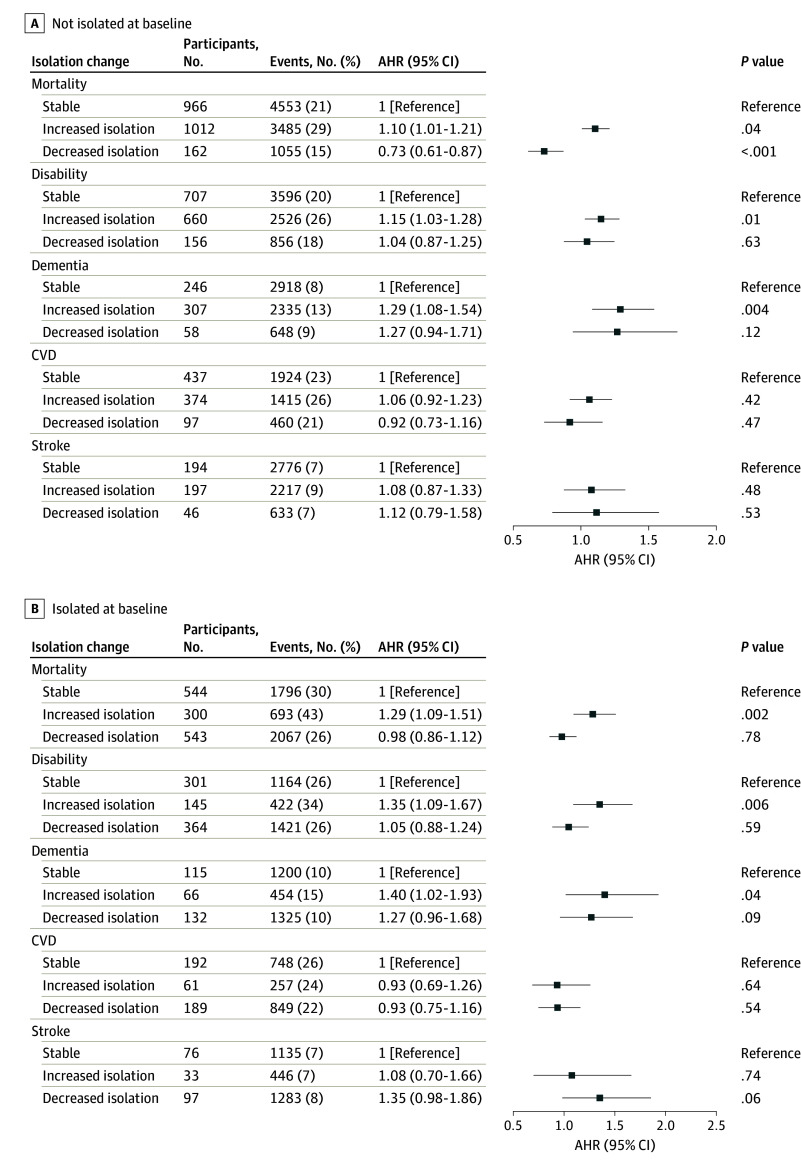
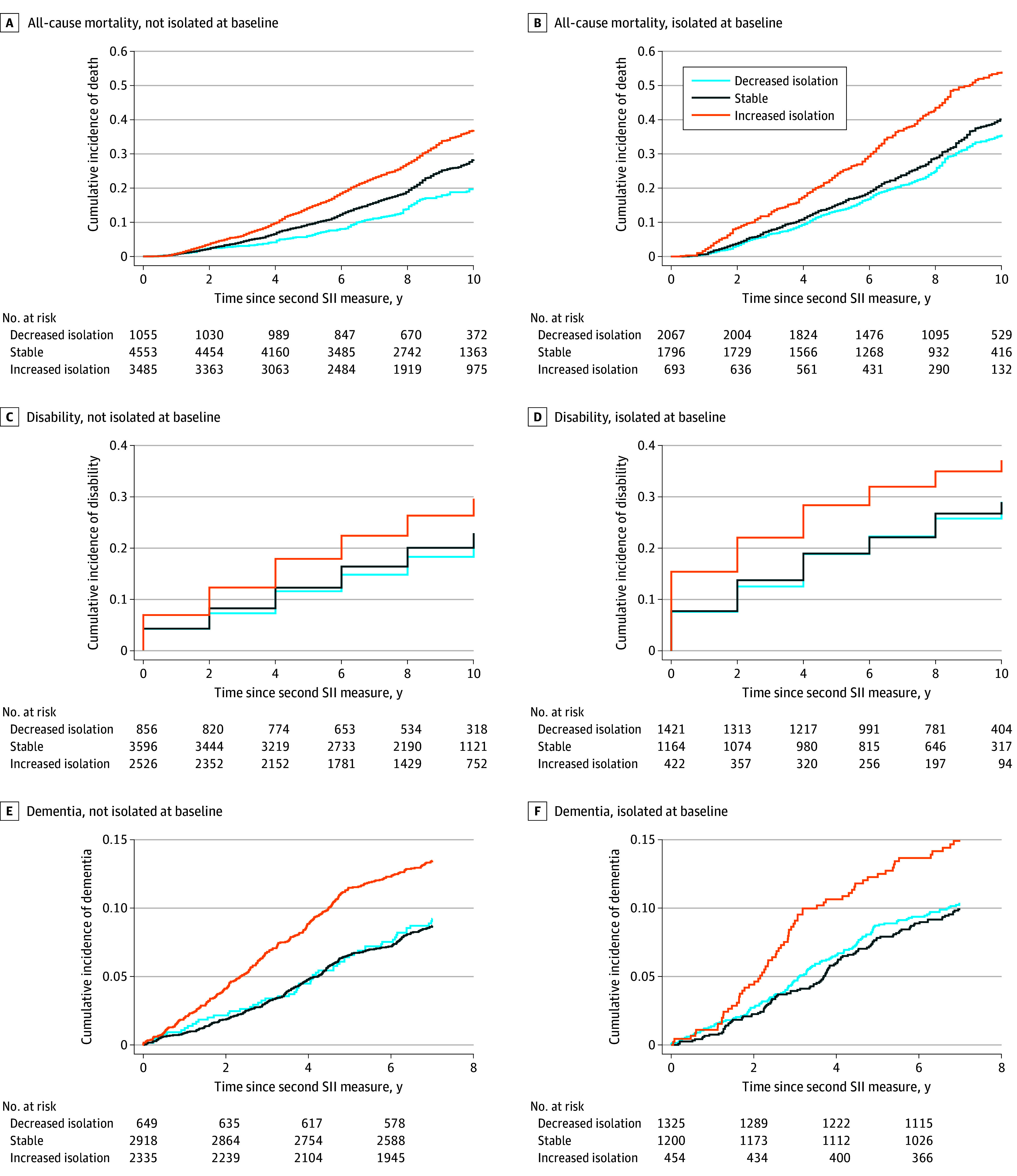
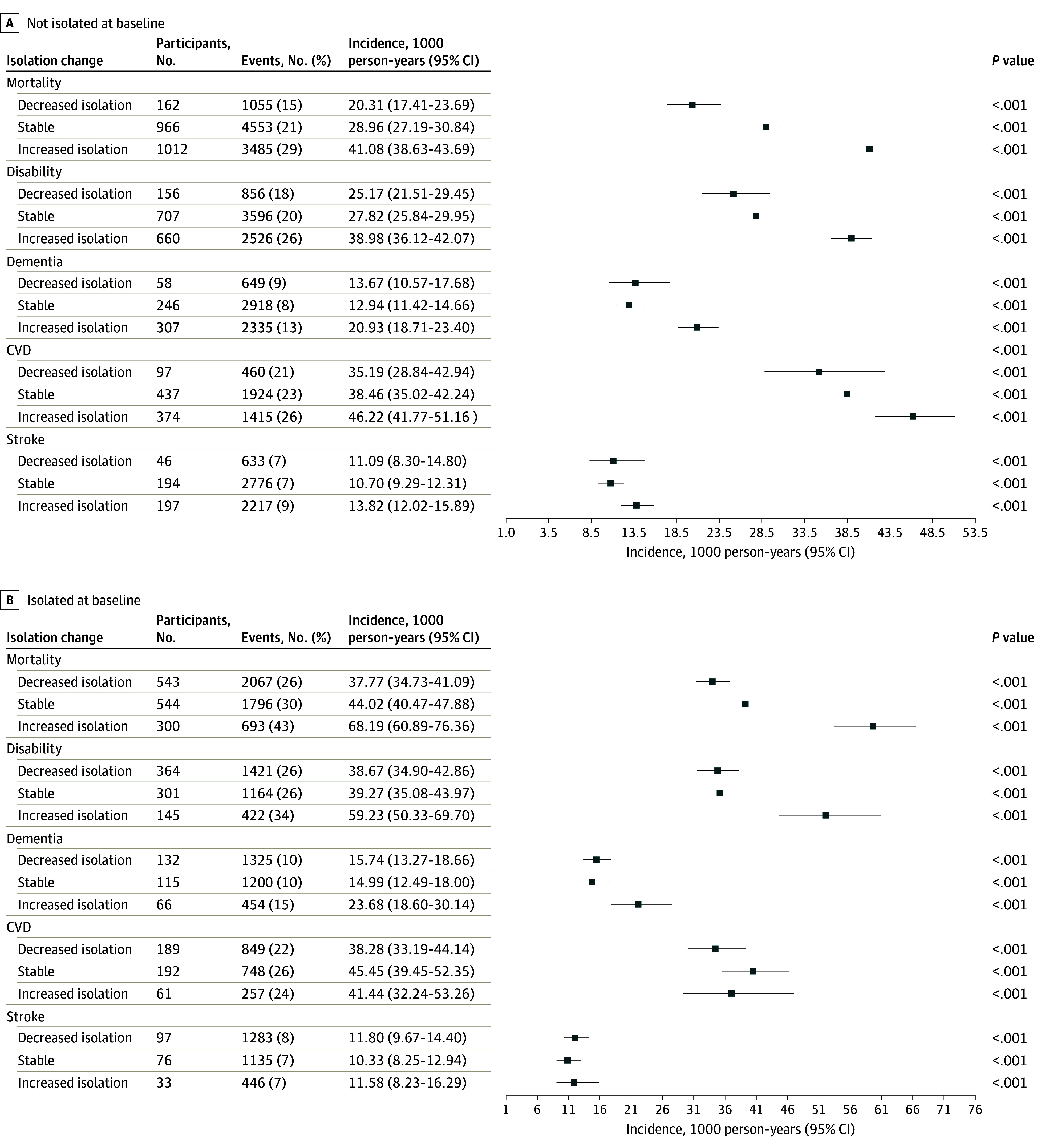
The primary outcomes were mortality, self-reported dependencies in activities of daily living, Alzheimer disease and Alzheimer disease-related dementia, CVD, and stroke. Dementia, CVD, and stroke were assessed using HRS-linked Medicare records. Incidence rates (IRs) of each group were estimated and a Cox proportional hazards regression model was used, with inverse-probability treatment weighting to adjust for confounders.
Among 13 649 participants (mean [SD] age at baseline, 65.3 [9.5] years; 8011 [58.7%] women) isolated at baseline, those with increased isolation had higher mortality (n = 693; IR = 68.19; 95% CI, 60.89-76.36 per 1000 person-years) than those who were stable (n = 1796; IR = 44.02; 95% CI, 40.47-47.88 person-years) or had decreased isolation (n = 2067; IR = 37.77; 95% CI, 34.73-41.09 person-years) isolation. Increased isolation was associated with higher risks of mortality (adjusted hazard ratio [AHR], 1.29; 95% CI, 1.09-1.51), disability (AHR, 1.35; 95% CI, 1.09-1.67), and dementia (AHR, 1.40; 95% CI, 1.02-1.93) compared with stable isolation. Similar findings were observed among socially nonisolated participants at baseline.
In this cohort study, increased isolation was associated with elevated risks of mortality, disability, and dementia, irrespective of baseline isolation status. These results underscore the importance of interventions targeting the prevention of increased isolation among older adults to mitigate its adverse effects on mortality, as well as physical and cognitive function decline.
虽然横断面测量的社会隔离与不良健康结果之间的关联已得到充分证实,但关于社会隔离变化与健康结果之间的关联知之甚少。
评估社会隔离的变化与死亡率、身体功能、认知功能、心血管疾病 (CVD) 和中风之间的关系。
设计、地点和参与者:在一项队列设计中,使用 2006 年至 2020 年波次的 13649 名符合条件的健康与退休研究 (HRS) 受访者的 4 年内社会隔离变化及其随后的死亡率和其他结果进行评估。数据分析于 2023 年 10 月 11 日至 2024 年 4 月 26 日进行。
主要暴露因素是通过 Steptoe 5 项社会隔离指数从初始评估到 4 年后的第二次评估来衡量的社会隔离变化。根据基线隔离状态,将参与者分为隔离程度降低、稳定或增加的组。
主要结局是死亡率、日常活动自理能力下降、阿尔茨海默病和阿尔茨海默病相关痴呆、CVD 和中风。使用 HRS 关联的医疗保险记录评估痴呆症、CVD 和中风。估计每个组的发病率 (IR),并使用 Cox 比例风险回归模型,使用逆概率治疗加权来调整混杂因素。
在基线时处于孤立状态的 13649 名参与者(平均[SD]年龄为 65.3[9.5]岁;8011[58.7%]名女性)中,与稳定组(n=1796;IR=44.02;95%CI,40.47-47.88 人年)或隔离程度降低组(n=2067;IR=37.77;95%CI,34.73-41.09 人年)相比,隔离程度增加的患者死亡率更高(n=693;IR=68.19;95%CI,60.89-76.36 人年)。与稳定隔离相比,隔离程度增加与更高的死亡率(调整后的危险比[AHR],1.29;95%CI,1.09-1.51)、残疾(AHR,1.35;95%CI,1.09-1.67)和痴呆(AHR,1.40;95%CI,1.02-1.93)风险相关。在基线时非社会孤立的参与者中也观察到类似的发现。
在这项队列研究中,与稳定隔离相比,隔离程度增加与死亡率、残疾和痴呆的风险增加相关,无论基线隔离状态如何。这些结果强调了针对老年人群体预防隔离程度增加的干预措施的重要性,以减轻其对死亡率以及身体和认知功能下降的不利影响。