Federal State Budget Institution National Medical Research Radiology Centre of the Ministry of Healthcare of the Russian Federation (FSBI NMRRC), Moscow, Russia.
Peoples' Friendship University of Russia, Moscow, Russia.
J Cardiothorac Surg. 2024 Jul 29;19(1):471. doi: 10.1186/s13019-024-02922-5.
Lung cancer, which is diagnosed two to three times more frequently in patients over the age of 70, is a leading cause of cancer-specific mortality. Given the elevated risk of morbidity and mortality, surgical intervention may not always be the most appropriate primary treatment option. This study aims to evaluate specific risk factors associated with postoperative morbidity and mortality in elderly patients and to optimize patient selection therefore improving surgical outcomes.
The study encompassed a cohort of 73 patients aged 75 and above who underwent surgical treatment for non-small cell lung cancer (NSCLC) at the Department of Thoracic Surgery of the P. Hertsen Moscow Oncological Research Institute between 2015 and 2021. All patients underwent preoperative evaluation, including PET/CT staging and functional assessment, carried out by a multidisciplinary team comprising thoracic surgeons, anesthesiologists, and other medical specialists.
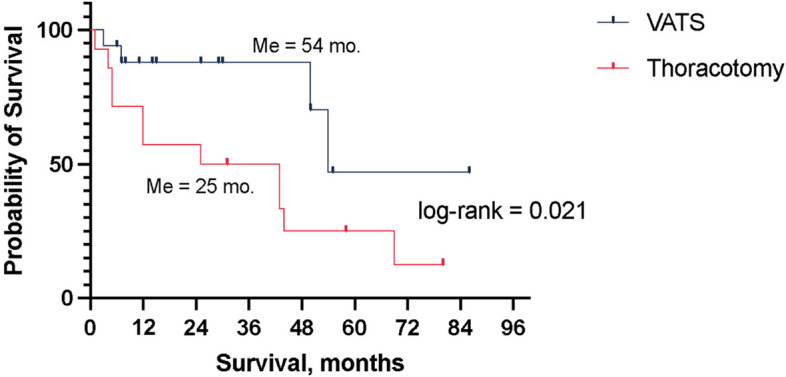
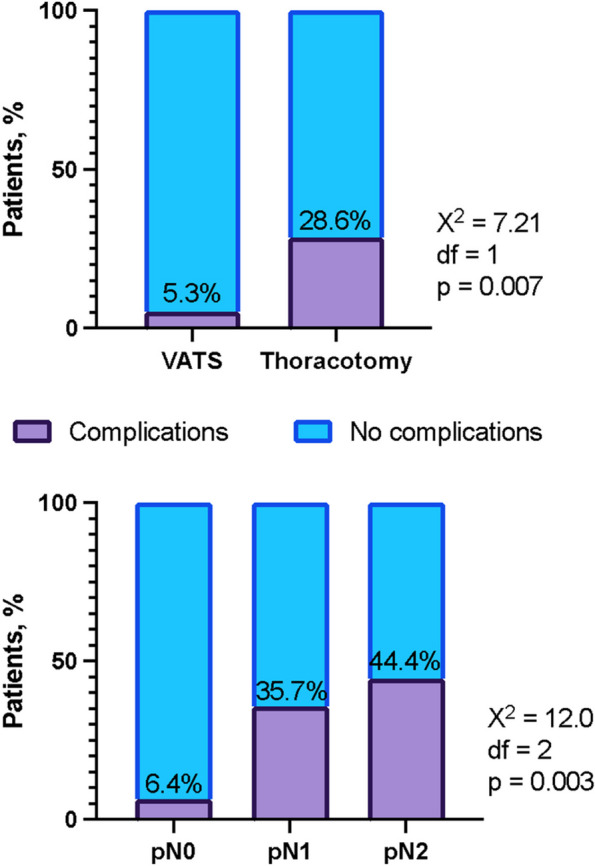
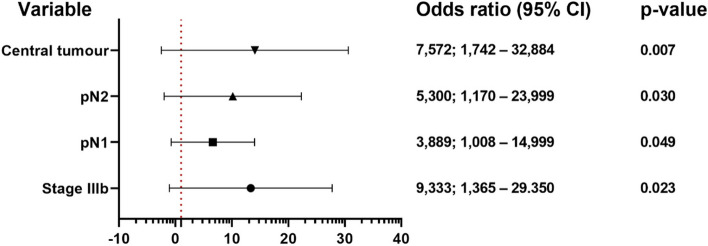
The investigation revealed a postoperative mortality rate of 5.5% and a postoperative morbidity incidence of 16.4%, with occurrences of atrial fibrillation in 41.6%, persistent air leak in 33.3%, and pneumonia in 25% of complicated cases. At the one-year follow-up, 88% of patients remained free from relapse, whereas at three years, this rate stood at 66%. During the follow-up period, 16 patients (22%) passed away, with a median survival duration of 44 months. Survival rates at one year, three years, and five years were 71%, 66%, and 35%, respectively. Multivariate analysis disclosed several significant factors predicting a complex postoperative period, including stage IIIb (p = 0.023), pN1 (p = 0.049), pN2 (p = 0.030), and central location (p = 0.007). Additionally, overall survival was primarily influenced by a Charlson comorbidity index of 6 (p = 0.044), stage Ia2 (p = 0.033), and the necessity for thoracotomy (p = 0.045).
Each case of lung cancer in patients aged 75 and older necessitates an individualized approach. Given the higher mortality rate relative to younger patients, comprehensive risk assessment and preoperative management of underlying comorbidities are imperative, with the involvement of anesthesiologists, intensive care physicians, cardiologists, and other relevant specialists as needed.
肺癌在 70 岁以上患者中的诊断频率要高出两到三倍,是癌症特异性死亡的主要原因。鉴于发病率和死亡率升高,手术干预可能并非总是最合适的主要治疗选择。本研究旨在评估与老年患者术后发病率和死亡率相关的特定风险因素,并因此优化患者选择,从而改善手术结果。
本研究纳入了 2015 年至 2021 年期间在莫斯科 P. Hertsen 肿瘤研究所胸外科接受非小细胞肺癌 (NSCLC) 手术治疗的 73 名 75 岁及以上的患者。所有患者均接受了多学科团队(包括胸外科医生、麻醉师和其他医学专家)进行的术前评估,包括 PET/CT 分期和功能评估。
研究显示,术后死亡率为 5.5%,术后发病率为 16.4%,并发症包括心房颤动 41.6%、持续性漏气 33.3%和肺炎 25%。在一年的随访中,88%的患者无复发,而三年时这一比例为 66%。随访期间,16 名患者(22%)死亡,中位生存期为 44 个月。一年、三年和五年的生存率分别为 71%、66%和 35%。多变量分析显示,IIIb 期(p=0.023)、pN1(p=0.049)、pN2(p=0.030)和中央位置(p=0.007)是预测术后复杂期的显著因素。此外,总生存主要受 Charlson 合并症指数为 6(p=0.044)、Ia2 期(p=0.033)和开胸手术必要性(p=0.045)的影响。
75 岁及以上老年患者的每例肺癌都需要个体化治疗。鉴于与年轻患者相比死亡率较高,因此需要进行全面的风险评估和术前合并症管理,必要时需要麻醉师、重症监护医生、心脏病专家和其他相关专家的参与。