Nasser Samar A, Arora Neha, Ferdinand Keith C
Department of Clinical Research & Leadership, School of Medicine and Health Sciences, The George Washington University, Washington, DC 20052, USA.
Department of Medicine, Tulane University School of Medicine, New Orleans, LA 70112, USA.
Rev Cardiovasc Med. 2022 Dec 19;23(12):411. doi: 10.31083/j.rcm2312411. eCollection 2022 Dec.
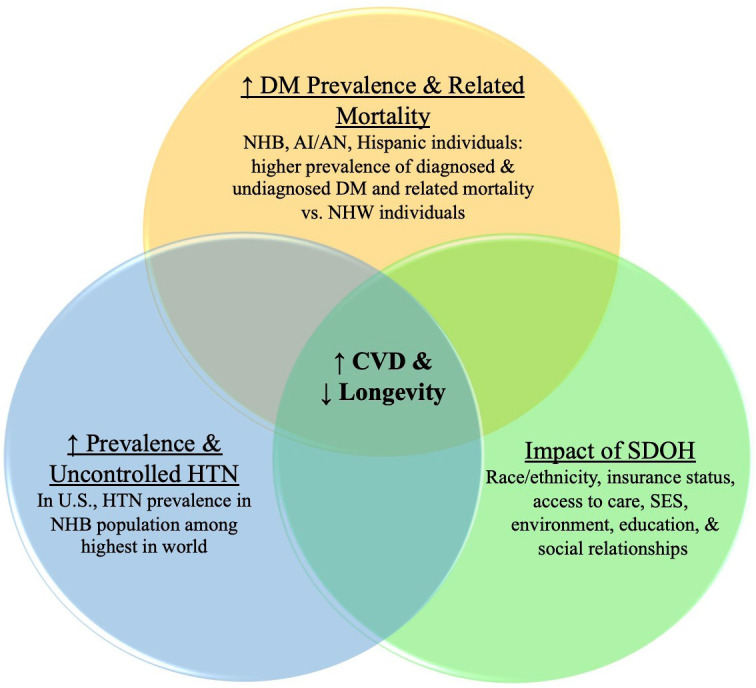
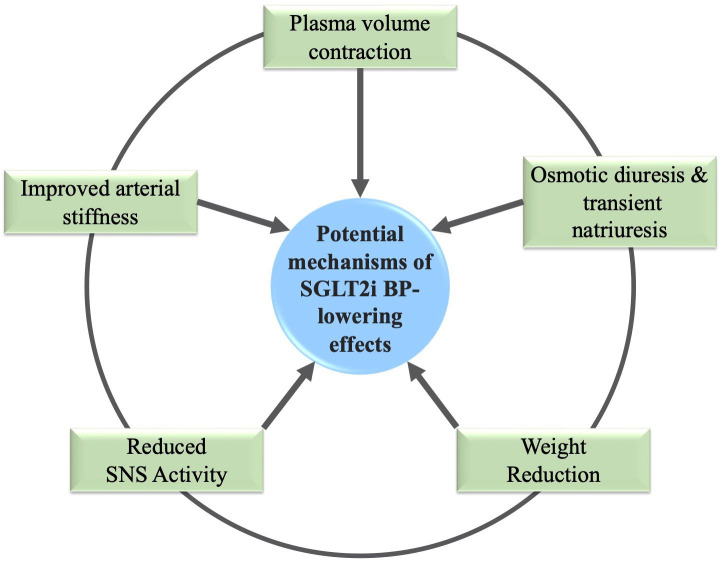
The racial/ethnic disparities in cardiometabolic risk factors and cardiovascular diseases (CVD) are prominent in non-Hispanic Black adults and other United States (U.S.) sub-populations, with evidence of differential access and quality of health care. High blood pressure (BP) is the most potent and prevalent risk factor for adverse cardiovascular (CV) outcomes across all populations globally, but especially in the non-Hispanic Black adults in the U.S. The use of sodium-glucose cotransporter-2 inhibitors (SGLT2is) demonstrate favorable effects in patients with and without type 2 diabetes (T2DM) in CVD especially for heart failure (HF), as the contemporary clinical practice recommendations and standards of care advocate. The beneficial effects of SGLT2is have been most profoundly documented with HF, including reduced (HFrEF) or preserved ejection fraction (HFpEF), and chronic kidney disease (CKD) with T2DM. Given that hypertension (HTN), CVD, HF, and CKD are significantly greater in certain racial/ethnic populations, the potential impact of SGLT2is will be more significant on the excess cardiometabolic and renal disease, especially in the Black patients. Moreover, there is a need for increased diverse representation in clinical trials. Inclusion of larger members of various racial/ethnic populations may assure that new and emerging data accurately reflect the diversity of the U.S. population. This review highlights potential benefits of SGLT2is, as noted in the most recent literature, and their BP-lowering impact on potentially reducing CV disparities, especially in Black adults. Furthermore, this commentary emphasizes the need to increase diversity in clinical trials to reduce the disparity gaps.
心血管代谢危险因素和心血管疾病(CVD)方面的种族/民族差异在非西班牙裔黑人成年人及美国其他亚人群体中十分突出,且有证据表明在获得医疗服务的机会和医疗质量方面存在差异。高血压(BP)是全球所有人群不良心血管(CV)结局中最具影响力且最普遍的危险因素,在美国非西班牙裔黑人成年人中尤为如此。使用钠-葡萄糖协同转运蛋白2抑制剂(SGLT2is)对患有和未患有2型糖尿病(T2DM)的CVD患者,尤其是心力衰竭(HF)患者显示出有益效果,正如当代临床实践建议和护理标准所倡导的那样。SGLT2is的有益作用在HF方面记录最为深刻,包括射血分数降低(HFrEF)或保留(HFpEF)以及T2DM合并慢性肾脏病(CKD)。鉴于高血压(HTN)、CVD、HF和CKD在某些种族/民族人群中更为显著,SGLT2is对过多的心血管代谢和肾脏疾病的潜在影响将更为显著,尤其是在黑人患者中。此外,临床试验中需要增加不同种族的代表性。纳入更多不同种族/民族人群的成员可以确保新出现的数据准确反映美国人群的多样性。本综述强调了SGLT2is的潜在益处,如最新文献中所述,及其对降低血压从而可能减少CV差异的影响,尤其是在黑人成年人中。此外,本评论强调需要增加临床试验的多样性以缩小差异差距。