Zhang Hongchen, Wang Yue, Zhang Xiaochen, Xu Chenshan, Xu Dongchao, Shen Hongzhang, Jin Hangbin, Yang Jianfeng, Zhang Xiaofeng
The Department of Gastroenterology, Affiliated Hangzhou First People's Hospital, School of Medicine, Westlake University, No. 261 HuanSha Road, Zhejiang, China.
The Fourth School of Clinical Medicine, Zhejiang Chinese Medical University, Hangzhou First People's Hospital, Hangzhou, 310003, China.
Antimicrob Resist Infect Control. 2024 Aug 7;13(1):84. doi: 10.1186/s13756-024-01441-1.
Endoscopic retrograde cholangiopancreatography (ERCP) has become a routine endoscopic procedure that is essential for diagnosing and managing various conditions, including gallstone extraction and the treatment of bile duct and pancreatic tumors. Despite its efficacy, post-ERCP infections - particularly those caused by carbapenem-resistant Enterobacterales (CRE) - present significant risks. These risks highlight the need for accurate predictive models to enhance postprocedural care, reduce the mortality risk associated with post-ERCP CRE sepsis, and improve patient outcomes in the context of increasing antibiotic resistance.
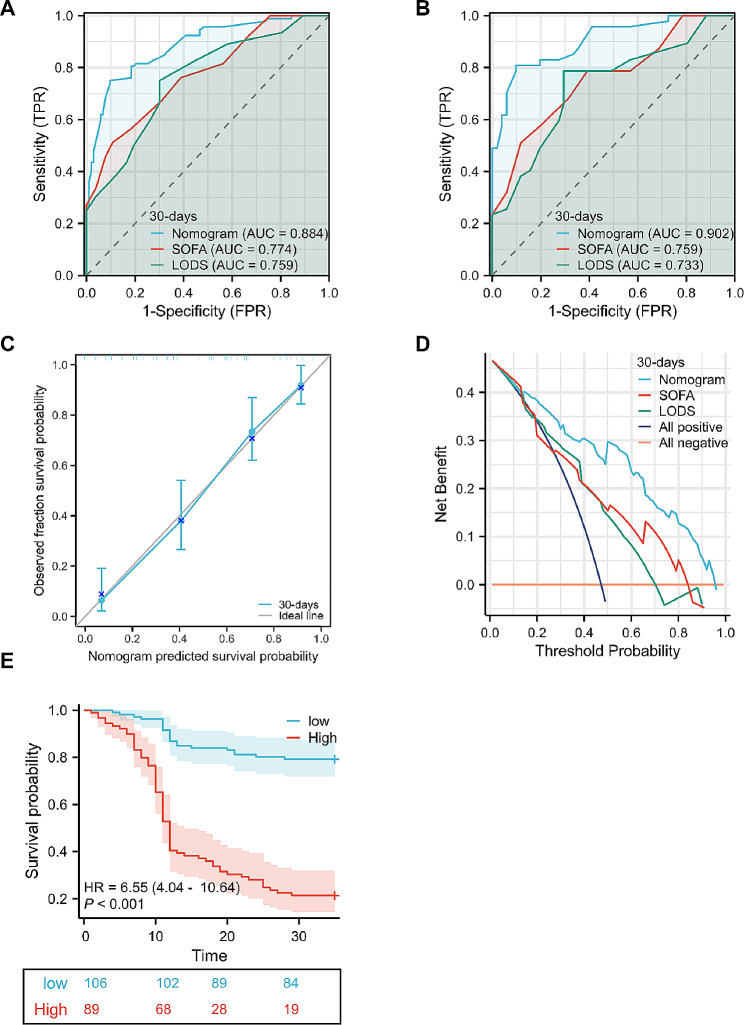
This study aimed to examine the risk factors for 30-day mortality in patients with CRE sepsis following ERCP and to develop a nomogram for accurately predicting 30-day mortality risk.
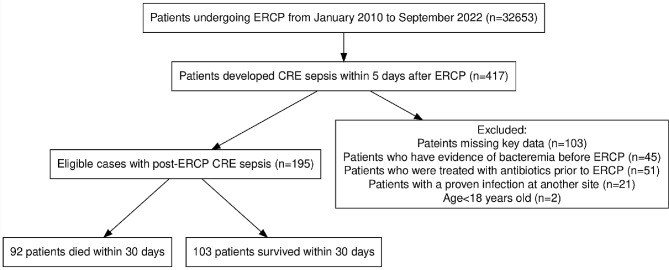
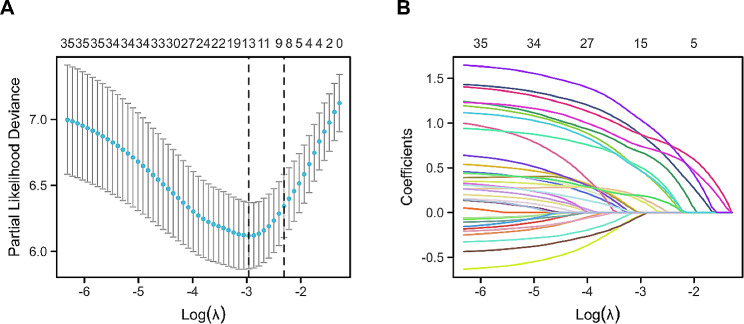
Data from 195 patients who experienced post-ERCP CRE sepsis between January 2010 and December 2022 were analyzed. Variable selection was optimized via the least absolute shrinkage and selection operator (LASSO) regression model. Multivariate logistic regression analysis was then employed to develop a predictive model, which was evaluated in terms of discrimination, calibration, and clinical utility. Internal validation was achieved through bootstrapping.
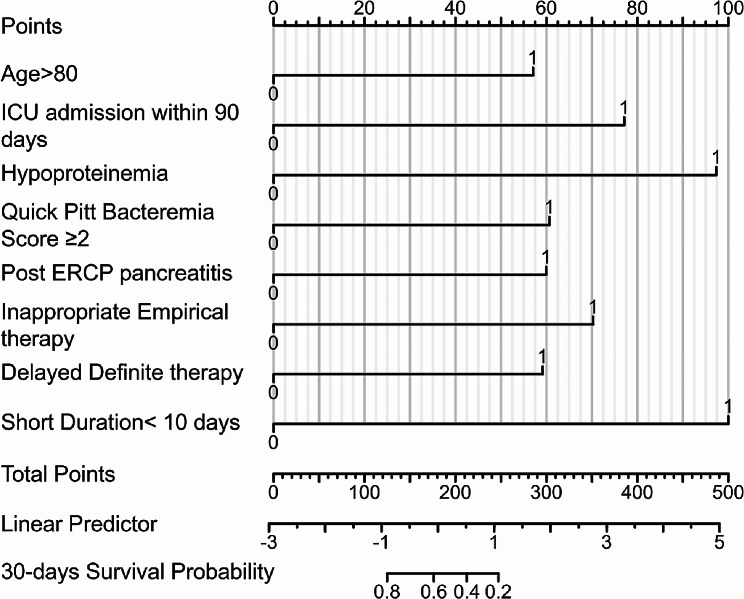
The nomogram included the following predictors: age > 80 years (hazard ratio [HR] 2.61), intensive care unit (ICU) admission within 90 days prior to ERCP (HR 2.64), hypoproteinemia (HR 4.55), quick Pitt bacteremia score ≥ 2 (HR 2.61), post-ERCP pancreatitis (HR 2.52), inappropriate empirical therapy (HR 3.48), delayed definitive therapy (HR 2.64), and short treatment duration (< 10 days) (HR 5.03). The model demonstrated strong discrimination and calibration.
This study identified significant risk factors associated with 30-day mortality in patients with post-ERCP CRE sepsis and developed a nomogram to accurately predict this risk. This tool enables healthcare practitioners to provide personalized risk assessments and promptly administer appropriate therapies against CRE, thereby reducing mortality rates.
内镜逆行胰胆管造影术(ERCP)已成为一种常规的内镜检查程序,对于诊断和管理各种病症至关重要,包括胆结石取出以及胆管和胰腺肿瘤的治疗。尽管其疗效显著,但ERCP术后感染——尤其是由耐碳青霉烯类肠杆菌科细菌(CRE)引起的感染——存在重大风险。这些风险凸显了需要准确的预测模型,以加强术后护理,降低与ERCP术后CRE败血症相关的死亡风险,并在抗生素耐药性增加的情况下改善患者预后。
本研究旨在探讨ERCP术后发生CRE败血症患者30天死亡率的危险因素,并开发一种列线图以准确预测30天死亡风险。
分析了2010年1月至2022年12月期间195例经历ERCP术后CRE败血症的患者的数据。通过最小绝对收缩和选择算子(LASSO)回归模型优化变量选择。然后采用多变量逻辑回归分析来开发预测模型,并从区分度、校准度和临床实用性方面进行评估。通过自举法实现内部验证。
列线图包括以下预测因素:年龄>80岁(风险比[HR]2.61)、ERCP术前90天内入住重症监护病房(ICU)(HR 2.64)、低蛋白血症(HR 4.55)、快速Pitt菌血症评分≥2(HR 2.61)、ERCP术后胰腺炎(HR 2.52)、经验性治疗不当(HR 3.48)、确定性治疗延迟(HR 2.64)以及治疗持续时间短(<10天)(HR 5.03)。该模型显示出很强的区分度和校准度。
本研究确定了与ERCP术后CRE败血症患者30天死亡率相关的重要危险因素,并开发了一种列线图以准确预测此风险。该工具使医疗保健从业者能够提供个性化的风险评估,并迅速针对CRE给予适当治疗,从而降低死亡率。