Pham Alex T, Pan Annabelle A, Bradley Chris, Hou Kaihua, Herbert Patrick, Johnson Chris, Wall Michael, Yohannan Jithin
Wilmer Eye Institute, Johns Hopkins University School of Medicine, Baltimore, MD, USA.
Malone Center for Engineering in Healthcare, Johns Hopkins University, Baltimore, MD, USA.
Transl Vis Sci Technol. 2024 Aug 1;13(8):12. doi: 10.1167/tvst.13.8.12.
Compare the use of optic disc and macular optical coherence tomography measurements to predict glaucomatous visual field (VF) worsening.
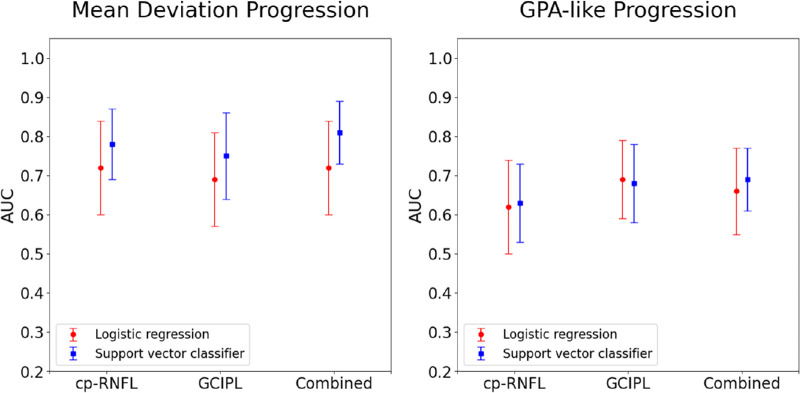
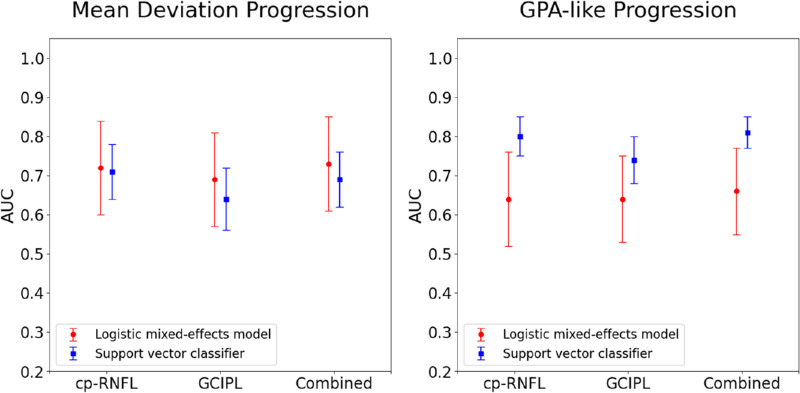
Machine learning and statistical models were trained on 924 eyes (924 patients) with circumpapillary retinal nerve fiber layer (cp-RNFL) or ganglion cell inner plexiform layer (GC-IPL) thickness measurements. The probability of 24-2 VF worsening was predicted using both trend-based and event-based progression definitions of VF worsening. Additionally, the cp-RNFL and GC-IPL predictions were combined to produce a combined prediction. A held-out test set of 617 eyes was used to calculate the area under the curve (AUC) to compare cp-RNFL, GC-IPL, and combined predictions.
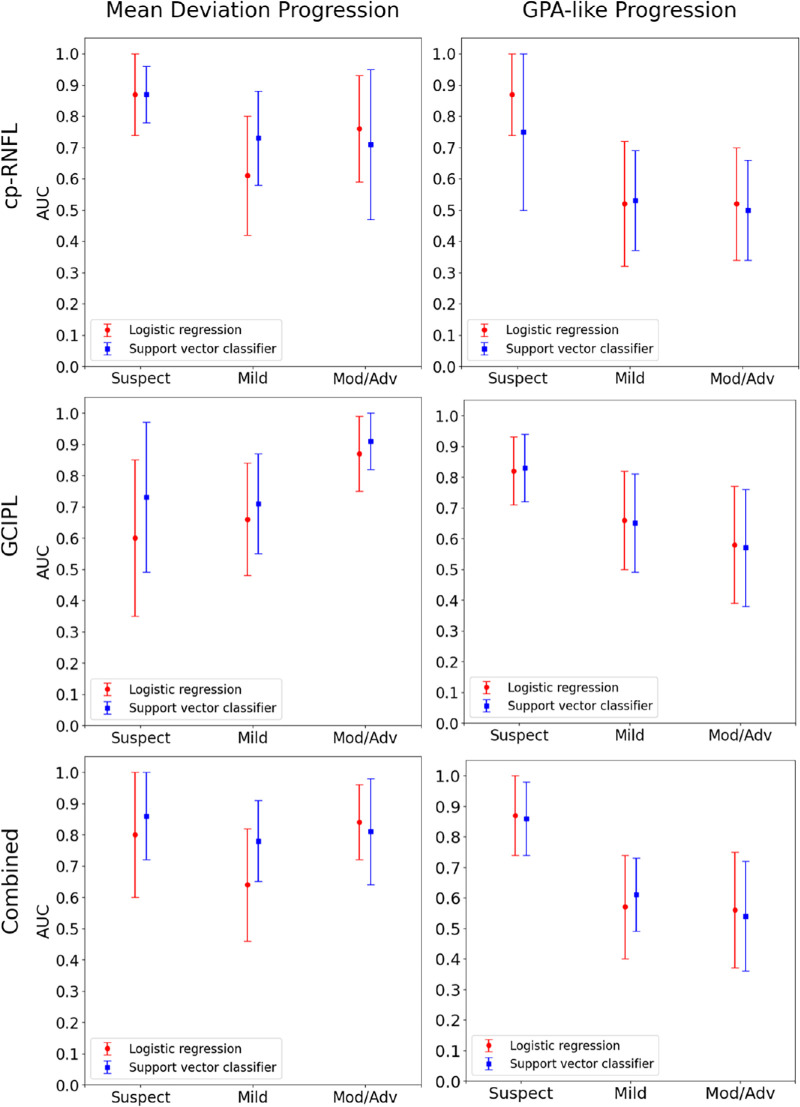
The AUCs for cp-RNFL, GC-IPL, and combined predictions with the statistical and machine learning models were 0.72, 0.69, 0.73, and 0.78, 0.75, 0.81, respectively, when using trend-based analysis as ground truth. The differences in performance between the cp-RNFL, GC-IPL, and combined predictions were not statistically significant. AUCs were highest in glaucoma suspects using cp-RNFL predictions and highest in moderate/advanced glaucoma using GC-IPL predictions. The AUCs for the statistical and machine learning models were 0.63, 0.68, 0.69, and 0.72, 0.69, 0.73, respectively, when using event-based analysis. AUCs decreased with increasing disease severity for all predictions.
cp-RNFL and GC-IPL similarly predicted VF worsening overall, but cp-RNFL performed best in early glaucoma stages and GC-IPL in later stages. Combining both did not enhance detection significantly.
cp-RNFL best predicted trend-based 24-2 VF progression in early-stage disease, while GC-IPL best predicted progression in late-stage disease. Combining both features led to minimal improvement in predicting progression.
比较视盘和黄斑光学相干断层扫描测量用于预测青光眼性视野(VF)恶化的情况。
对924只眼(924例患者)进行机器学习和统计模型训练,这些患者有视乳头周围视网膜神经纤维层(cp-RNFL)或神经节细胞内丛状层(GC-IPL)厚度测量值。使用基于趋势和基于事件的VF恶化进展定义来预测24-2 VF恶化的概率。此外,将cp-RNFL和GC-IPL预测结果相结合以产生联合预测。使用617只眼的保留测试集来计算曲线下面积(AUC),以比较cp-RNFL、GC-IPL和联合预测结果。
当使用基于趋势的分析作为金标准时,cp-RNFL、GC-IPL以及联合统计模型和机器学习模型的预测的AUC分别为0.72、0.69、0.73以及0.78、0.75、0.81。cp-RNFL、GC-IPL和联合预测之间的性能差异无统计学意义。在青光眼可疑患者中,使用cp-RNFL预测时AUC最高,在中度/重度青光眼患者中,使用GC-IPL预测时AUC最高。当使用基于事件的分析时,统计模型和机器学习模型的AUC分别为0.63、0.68、0.69以及0.72、0.69、0.73。所有预测的AUC均随疾病严重程度增加而降低。
cp-RNFL和GC-IPL总体上对VF恶化的预测相似,但cp-RNFL在青光眼早期阶段表现最佳,而GC-IPL在后期阶段表现最佳。两者结合并不能显著提高检测效果。
cp-RNFL最能预测早期疾病中基于趋势的24-2 VF进展,而GC-IPL最能预测晚期疾病的进展。结合这两个特征在预测进展方面的改善最小。