Department of Minimally Invasive Interventional Therapy, State Key Laboratory of Oncology in South China, Guangdong Provincial Clinical Research Center for Cancer, Sun Yat-sen University Cancer Center, Guangzhou, China.
Department of Interventional Radiology, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, China.
Front Immunol. 2024 Jul 26;15:1430571. doi: 10.3389/fimmu.2024.1430571. eCollection 2024.
Intermediate-stage (BCLC-B) hepatocellular carcinoma (HCC) beyond the up-to-11 criteria represent a significant therapeutic challenge due to high and heterogeneous tumor burden. This study evaluated the effectiveness and safety of transarterial chemoembolization (TACE) in combination with lenvatinib and tislelizumab for these patients.
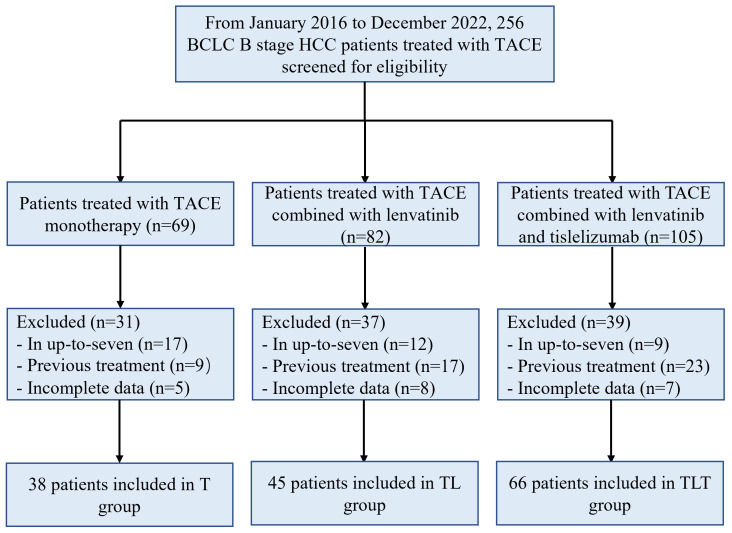
In this retrospective cohort study, patients with unresectable intermediate-stage HCC beyond the up-to-11 criteria were enrolled and divided into TACE monotherapy (T), TACE combined with lenvatinib (TL), or TACE plus lenvatinib and tislelizumab (TLT) group based on the first-line treatment, respectively. The primary endpoint was overall survival (OS). The secondary outcomes included progression-free survival (PFS), tumor response according to RESIST1.1 and modified RECIST, and adverse events (AEs).
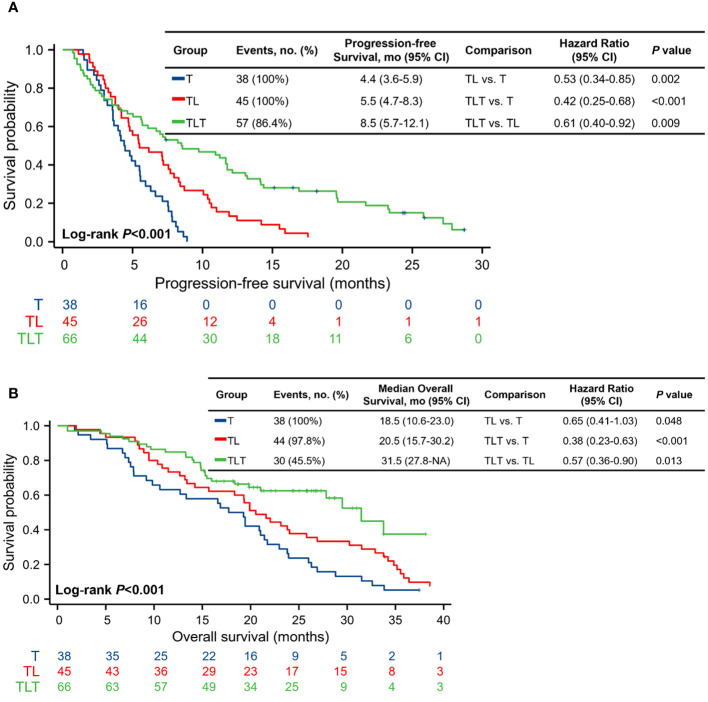
There were 38, 45, and 66 patients in the T, TL, and TLT groups, respectively. The TLT group exhibited significantly higher ORR and DCR than the other two groups, as assessed by either mRECIST or RECIST 1.1 (all <0.05). Median PFS and OS were significantly longer in the TLT group compared with the T group (PFS: 8.5 vs. 4.4 months; OS: 31.5 vs. 18.5 months; all <0.001) and TL group (PFS: 8.5 vs. 5.5 months; OS: 31.5 vs. 20.5 months; all <0.05). The incidence of TRAEs was slightly higher in the TLT and TL groups than in the T group, while all the toxicities were tolerable. No treatment-related death occurred in all groups.
TACE combined with lenvatinib and tislelizumab significantly improved the survival benefit compared with TACE monotherapy and TACE plus lenvatinib in patients with intermediate-stage HCC beyond the up-to-11 criteria, with an acceptable safety profile.
超出 up-to-11 标准的中期(BCLC-B)肝细胞癌(HCC)由于肿瘤负荷高且异质性大,是一个重大的治疗挑战。本研究评估了经动脉化疗栓塞(TACE)联合仑伐替尼和替雷利珠单抗治疗这些患者的有效性和安全性。
在这项回顾性队列研究中,招募了不符合 up-to-11 标准的不可切除的中期 HCC 患者,并根据一线治疗方案将其分为 TACE 单药治疗(T)、TACE 联合仑伐替尼(TL)或 TACE 联合仑伐替尼和替雷利珠单抗(TLT)组。主要终点是总生存期(OS)。次要结局包括无进展生存期(PFS)、根据 RESIST1.1 和改良 RECIST 评估的肿瘤缓解率、以及不良事件(AEs)。
T、TL 和 TLT 组分别有 38、45 和 66 例患者。TLT 组的客观缓解率(ORR)和疾病控制率(DCR)明显高于其他两组,无论是根据 mRECIST 还是 RECIST 1.1 评估(均<0.05)。TLT 组的中位 PFS 和 OS 明显长于 T 组(PFS:8.5 与 4.4 个月;OS:31.5 与 18.5 个月;均<0.001)和 TL 组(PFS:8.5 与 5.5 个月;OS:31.5 与 20.5 个月;均<0.05)。TLT 组和 TL 组的 TRAE 发生率略高于 T 组,但所有毒性均可耐受。所有组均未发生治疗相关死亡。
TACE 联合仑伐替尼和替雷利珠单抗可显著提高超出 up-to-11 标准的中期 HCC 患者的生存获益,优于 TACE 单药治疗和 TACE 联合仑伐替尼治疗,且安全性可接受。