Department of Internal Medicine, National Taiwan University Hospital, Yun-Lin Branch, Yunlin County, Taiwan.
Graduate Institute of Clinical Medicine, College of Medicine, National Taiwan University, 7 Chung-Shan South Road, Taipei, 100, Taiwan (ROC).
Respir Res. 2024 Aug 14;25(1):308. doi: 10.1186/s12931-024-02931-x.
Airflow obstruction is a hallmark of disease severity and prognosis in bronchiectasis. The relationship between lung microbiota, airway inflammation, and outcomes in bronchiectasis with fixed airflow obstruction (FAO) remains unclear. This study explores these interactions in bronchiectasis patients, with and without FAO, and compares them to those diagnosed with chronic obstructive pulmonary disease (COPD).
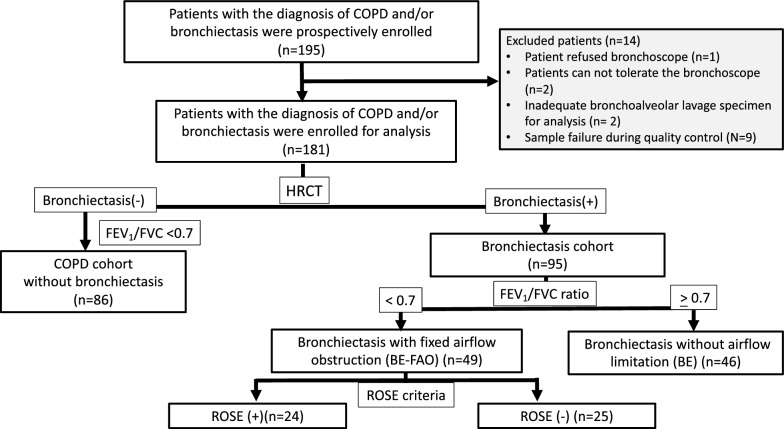
This prospective observational study in Taiwan enrolled patients with either bronchiectasis or COPD. To analyze the lung microbiome and assess inflammatory markers, bronchoalveolar lavage (BAL) samples were collected for 16S rRNA gene sequencing. The study cohort comprised 181 patients: 86 with COPD, 46 with bronchiectasis, and 49 with bronchiectasis and FAO, as confirmed by spirometry.
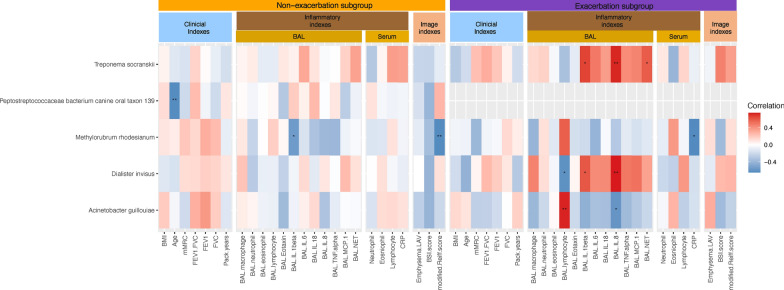
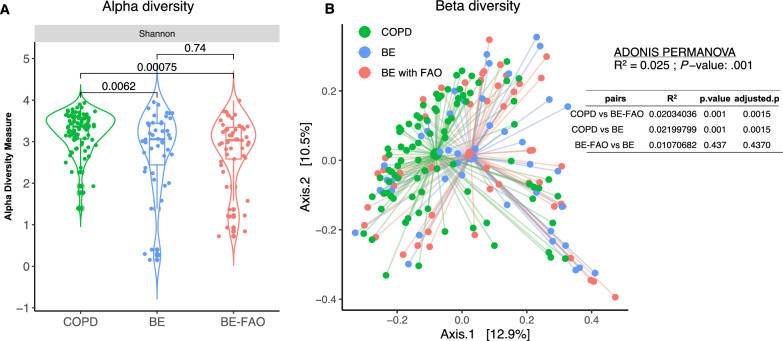
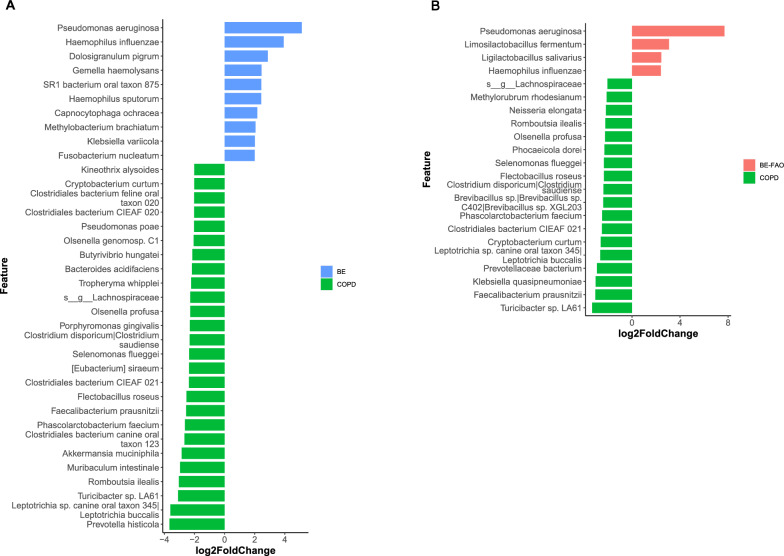
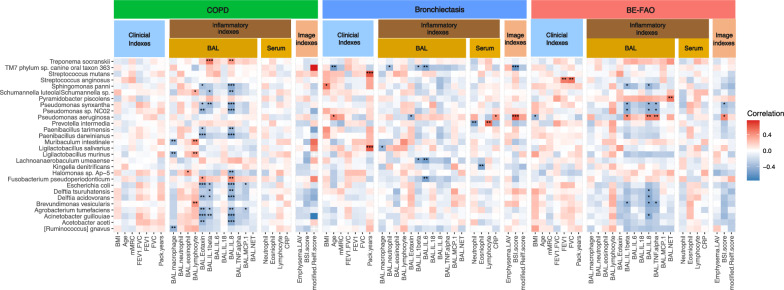
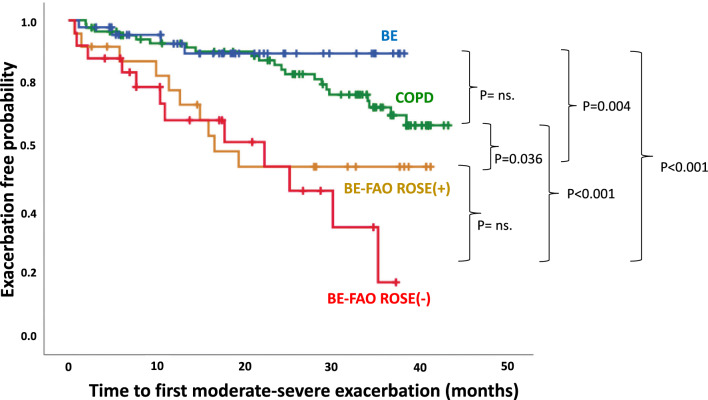
Patients with bronchiectasis, with or without FAO, had similar microbiome profiles characterized by reduced alpha diversity and a predominance of Proteobacteria, distinctly different from COPD patients who exhibited more Firmicutes, greater diversity, and more commensal taxa. Furthermore, compared to COPD and bronchiectasis without FAO, bronchiectasis with FAO showed more severe disease and a higher risk of exacerbations. A significant correlation was found between the presence of Pseudomonas aeruginosa and increased airway neutrophilic inflammation such as Interleukin [IL]-1β, IL-8, and tumor necrosis factor-alpha [TNF]-α, as well as with higher bronchiectasis severity, which might contribute to an increased risk of exacerbations. Moreover, in bronchiectasis patients with FAO, the ROSE (Radiology, Obstruction, Symptoms, and Exposure) criteria were employed to classify individuals as either ROSE (+) or ROSE (-), based on smoking history. This classification highlighted differences in clinical features, inflammatory profiles, and slight microbiome variations between ROSE (-) and ROSE (+) patients, suggesting diverse endotypes within the bronchiectasis with FAO group.
Bronchiectasis patients with FAO may exhibit two distinct endotypes, as defined by ROSE criteria, characterized by greater disease severity and a lung microbiome more similar to bronchiectasis without FAO than to COPD. The significant correlation between Pseudomonas aeruginosa colonization and increased airway neutrophilic inflammation, as well as disease severity, underscores the clinical relevance of microbial patterns. This finding reinforces the potential role of these patterns in the progression and exacerbations of bronchiectasis with FAO.
气流阻塞是支气管扩张症严重程度和预后的标志。在有固定气流阻塞(FAO)的支气管扩张症患者中,肺部微生物群、气道炎症与结局之间的关系尚不清楚。本研究旨在探讨有无 FAO 的支气管扩张症患者的这些相互作用,并将其与慢性阻塞性肺疾病(COPD)患者进行比较。
本研究在台湾进行,纳入了支气管扩张症或 COPD 患者。为了分析肺部微生物群并评估炎症标志物,对支气管肺泡灌洗液(BAL)样本进行了 16S rRNA 基因测序。研究队列包括 181 名患者:86 名 COPD 患者、46 名支气管扩张症患者和 49 名支气管扩张症合并 FAO 患者,通过肺量测定法进行确诊。
有或无 FAO 的支气管扩张症患者的微生物群特征相似,表现为α多样性降低,优势菌为变形菌门,与 COPD 患者明显不同,后者表现为厚壁菌门更多、多样性更大、共生菌更多。此外,与 COPD 和无 FAO 的支气管扩张症患者相比,有 FAO 的支气管扩张症患者的疾病更严重,发生加重的风险更高。与气道中性粒细胞炎症标志物(如白细胞介素[IL]-1β、IL-8 和肿瘤坏死因子-α[TNF]-α)的增加一样,铜绿假单胞菌的存在与支气管扩张症的严重程度呈显著正相关,这可能会增加加重的风险。此外,在有 FAO 的支气管扩张症患者中,根据吸烟史,采用 ROSE(放射学、阻塞、症状和暴露)标准将患者分为 ROSE(+)或 ROSE(-)。这种分类突出了 ROSE(-)和 ROSE(+)患者之间临床特征、炎症谱和轻微微生物群差异,表明有 FAO 的支气管扩张症患者可能存在两种不同的表型,这两种表型与无 FAO 的支气管扩张症患者更相似,而与 COPD 患者不同。铜绿假单胞菌定植与气道中性粒细胞炎症增加以及疾病严重程度之间的显著相关性突出了微生物群模式的临床相关性。这一发现强化了这些模式在有 FAO 的支气管扩张症的进展和加重中的潜在作用。