Goldstein Stuart L, Akcan-Arikan Ayse, Afonso Natasha, Askenazi David J, Basalely Abby M, Basu Rajit K, Beng Hostensia, Fitzgerald Julie C, Gist Katja, Kizilbash Sarah, Kwiatkowski David, Mastropietro Christopher W, Menon Shina, SooHoo Megan, Traum Avram Z, Bird Christopher A
Cincinnati Children's Hospital Medical Center, University of Cincinnati College of Medicine, Cincinnati, Ohio, USA.
University of Cincinnati College of Medicine, Cincinnati, Ohio, USA.
Kidney Int Rep. 2024 May 15;9(8):2443-2452. doi: 10.1016/j.ekir.2024.05.010. eCollection 2024 Aug.
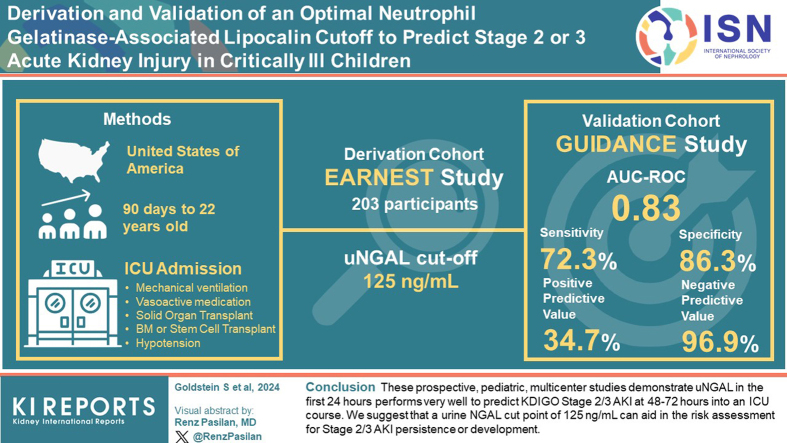
Acute kidney injury (AKI) defined by changes in serum creatinine (SCr), or oliguria is associated with increased morbidity and mortality in children who are critically ill. We derived and validated a clinical cutoff value for urine neutrophil gelatinase-associated lipocalin (NGAL), in a prospective multicenter study of children who were critically ill. We report the clinical performance of urine NGAL (uNGAL) to aid in pediatric AKI risk assessment.
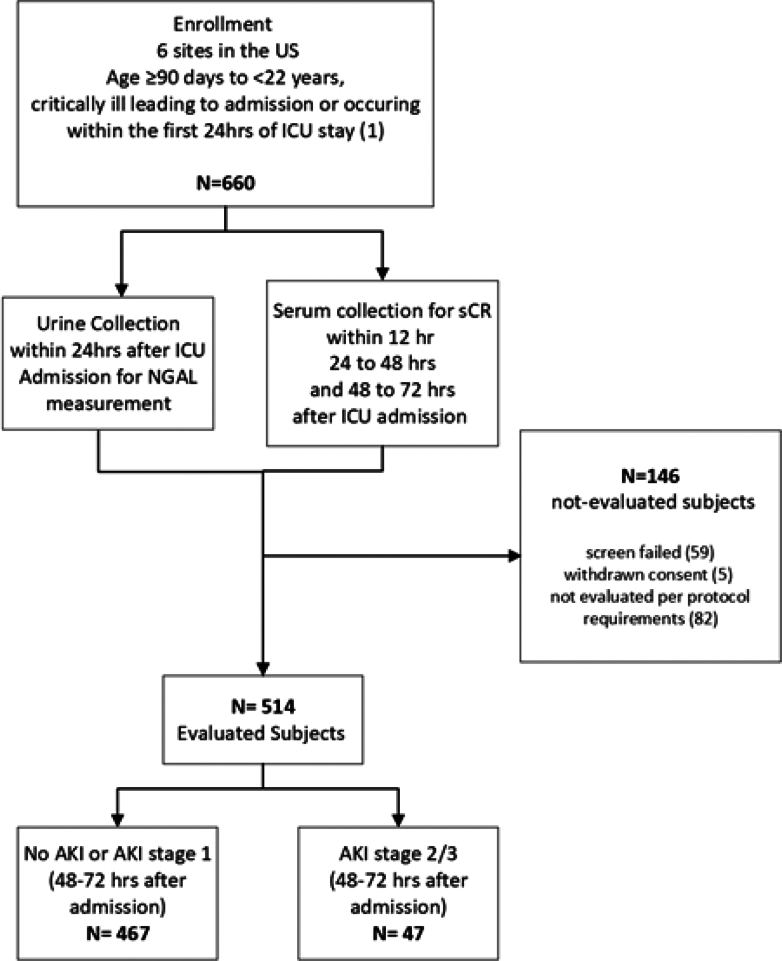
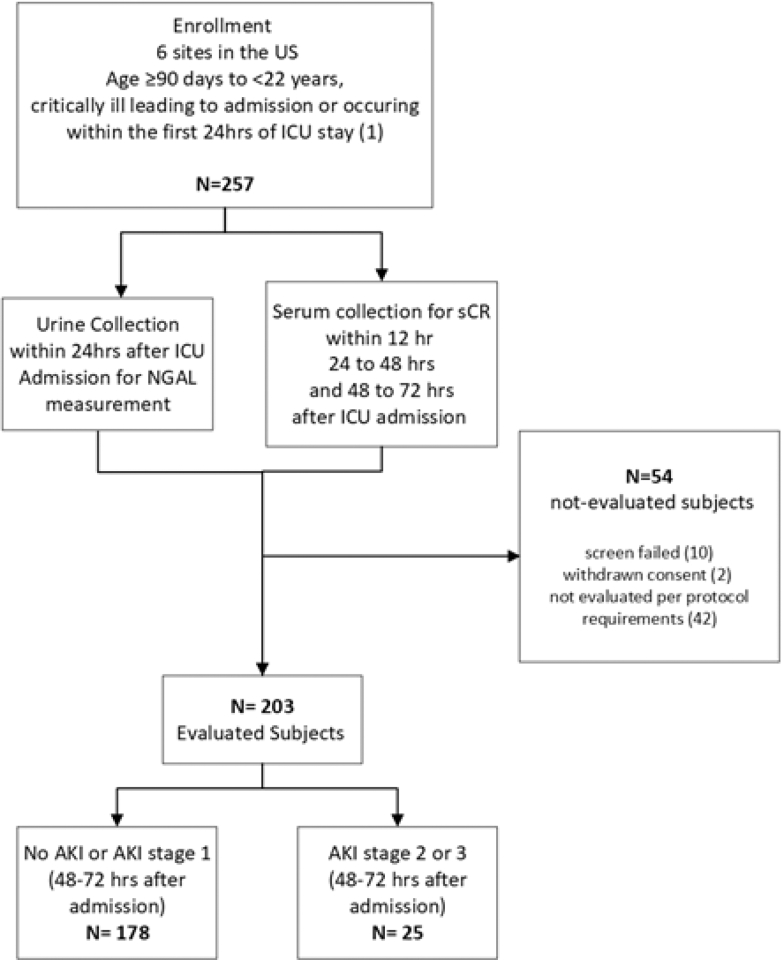
Eligible subjects were aged ≥ 90 days to < 22 years, admitted to an intensive care unit (ICU), and had 1 or more of the following: mechanical ventilation, vasoactive medication administration, solid organ or bone marrow transplantation, or hypotension within 24-hours of admission. uNGAL was assessed within 24-hours of admission. The primary outcome was SCr-based stage 2/3 AKI presence at 48- to 72-hours.
Twenty-five (12.3%) derivation study patients had stage 2/3 AKI at 48- to 72-hours. uNGAL concentration of 125 ng/ml was the optimal cutoff. Forty-seven (9.1%) validation study patients had stage 2/3 AKI at 48- to 72-hours. The area under the curve of a receiver operator characteristics curve (AUC-ROC) for uNGAL performance was 0.83 (95% confidence interval [CI]: 0.77-0.90). Performance characteristics were sensitivity 72.3% (95% CI: 57.4%-84.4%), specificity 86.3% (95% CI: 82.8%-89.3%), positive predictive value 34.7% (95% CI: 28.5%-41.5%), and negative predictive value 96.9% (95% CI: 95.1%-98.0%).
These prospective, pediatric, multicenter studies demonstrate that uNGAL in the first 24-hours performs very well to predict Kidney Disease Improving Global Outcomes (KDIGO) stage 2/3 AKI at 48- to 72-hours into an ICU course. We suggest that a uNGAL cut point of 125 ng/ml can aid in the risk assessment for stage 2/3 AKI persistence or development.
由血清肌酐(SCr)变化或少尿定义的急性肾损伤(AKI)与危重症儿童的发病率和死亡率增加相关。在一项针对危重症儿童的前瞻性多中心研究中,我们推导并验证了尿中性粒细胞明胶酶相关脂质运载蛋白(NGAL)的临床临界值。我们报告了尿NGAL(uNGAL)在儿科AKI风险评估中的临床表现。
符合条件的受试者年龄≥90天至<22岁,入住重症监护病房(ICU),且在入院后24小时内有以下1项或多项情况:机械通气、血管活性药物给药、实体器官或骨髓移植或低血压。在入院后24小时内评估uNGAL。主要结局是在48至72小时时基于SCr的2/3期AKI的存在情况。
25名(12.3%)推导研究患者在48至72小时时患有2/3期AKI。uNGAL浓度为125 ng/ml是最佳临界值。47名(9.1%)验证研究患者在48至72小时时患有2/3期AKI。uNGAL表现的受试者工作特征曲线(AUC-ROC)下面积为0.83(95%置信区间[CI]:0.77-0.90)。性能特征为敏感性72.3%(95%CI:57.4%-84.4%),特异性86.3%(95%CI:82.8%-89.3%),阳性预测值34.7%(95%CI:28.5%-41.5%),阴性预测值96.9%(95%CI:95.1%-98.0%)。
这些前瞻性、儿科、多中心研究表明,在入住ICU病程的48至72小时内,最初24小时的uNGAL在预测改善全球肾脏病预后(KDIGO)2/3期AKI方面表现良好。我们建议uNGAL切点为125 ng/ml有助于2/3期AKI持续存在或发展的风险评估。