Department of Medical and Surgical Sciences, Alma Mater Studiorum, University of Bologna, Bologna, Italy.
Clinical Pharmacology Unit, Department for Integrated Infectious Risk Management, IRCCS Azienda Ospedaliero-Universitaria di Bologna, 40138, Bologna, Italy.
Clin Pharmacokinet. 2024 Sep;63(9):1271-1282. doi: 10.1007/s40262-024-01410-2. Epub 2024 Aug 22.
Dalbavancin is increasingly used for the long-term treatment of chronic osteoarticular infections. A population pharmacokinetic/pharmacodynamic (PK/PD) analysis for assessing the relationship between dalbavancin exposure and C-reactive protein (C-RP) over time was conducted.
Non-linear mixed-effect modeling was fitted to dalbavancin and C-RP concentrations. Monte Carlo simulations assessed the weekly percentage of C-RP reduction associated with different dosing regimens, starting from baseline to < 1 mg/dL.
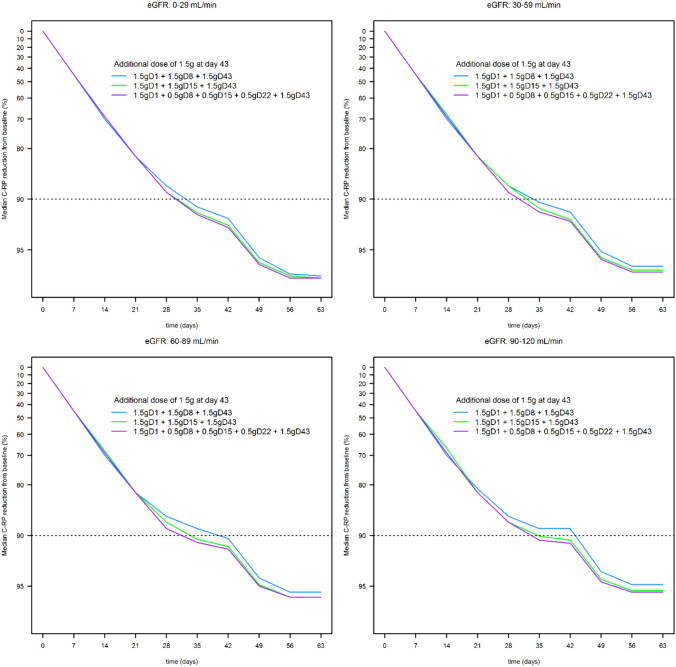
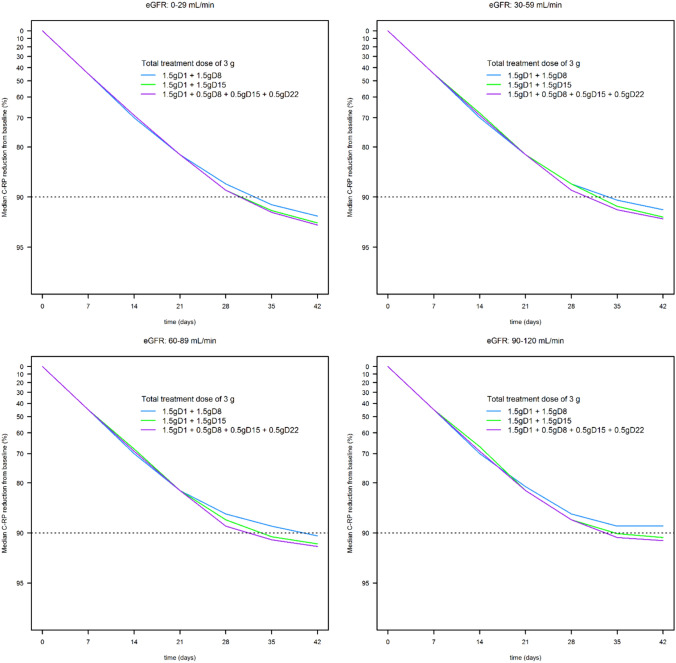
A total of 45 patients were retrospectively included in the analysis. The PK of dalbavancin was described by a two-compartment model, and the PD of C-RP was described by an indirect turnover maximum inhibition model. The total dalbavancin concentration model estimate producing 50% of maximum C-RP production inhibition (IC) was 0.70 mg/L. Monte Carlo simulations showed that in patients with staphylococcal osteoarticular infections targeting total dalbavancin concentrations at > 14.5 mg/L at any time point may achieve C-RP production inhibition over time in > 95% of patients. Based on this, the findings showed that a cumulative dose of 3000 mg administered in the first 3 weeks may lead to a > 90% C-RP decrease versus baseline in approximately 5-6 weeks. In patients needing treatment prolongation, an additional 1500 mg dose after this period may maintain C-RP concentrations < 1 mg/dL for other 3 weeks.
A decrease in C-RP is related to dalbavancin exposure in osteoarticular infections. Targeting dalbavancin plasma concentrations above the efficacy threshold may be associated with effective treatment.
达巴万星被越来越多地用于慢性骨关节炎感染的长期治疗。进行了一项群体药代动力学/药效学(PK/PD)分析,以评估达巴万星暴露与 C 反应蛋白(C-RP)随时间的关系。
采用非线性混合效应模型拟合达巴万星和 C-RP 浓度。蒙特卡罗模拟评估了不同给药方案从基线开始至 < 1 mg/dL 时与 C-RP 降低相关的每周百分比。
共回顾性纳入 45 例患者进行分析。达巴万星 PK 采用双室模型描述,C-RP PD 采用间接转换最大抑制模型描述。产生最大 C-RP 产生抑制 50%的总达巴万星浓度模型估算值为 0.70 mg/L。蒙特卡罗模拟表明,在金黄色葡萄球菌骨关节炎感染患者中,任何时间点的总达巴万星浓度目标值>14.5 mg/L 可能会使 C-RP 产生抑制随时间推移在>95%的患者中实现。基于此,结果表明在第 3 周内给予 3000 mg 的累积剂量可能会导致约 5-6 周内 C-RP 相对于基线降低>90%。对于需要延长治疗的患者,在此期间后额外给予 1500 mg 剂量可能会使 C-RP 浓度在另外 3 周内保持 < 1 mg/dL。
C-RP 的降低与骨关节炎感染中的达巴万星暴露有关。将达巴万星血浆浓度靶向高于疗效阈值可能与有效治疗相关。