Department of Emergency and Critical Care Medicine, Osaka Medical and Pharmaceutical University, Takatsuki, Osaka, Japan.
Division of Trauma and Surgical Critical Care, Osaka General Medical Center, Sumiyoshi-ku, Osaka, Japan.
Crit Care Explor. 2024 Aug 26;6(9):e1142. doi: 10.1097/CCE.0000000000001142. eCollection 2024 Sep 1.
This study aimed to elucidate the association between IV contrast media CT and acute kidney injury (AKI) and in-hospital mortality among patients requiring emergency admission.
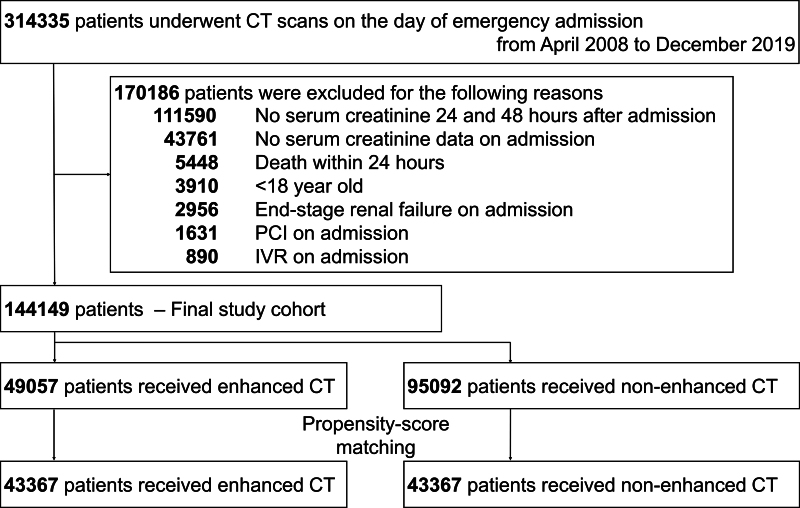
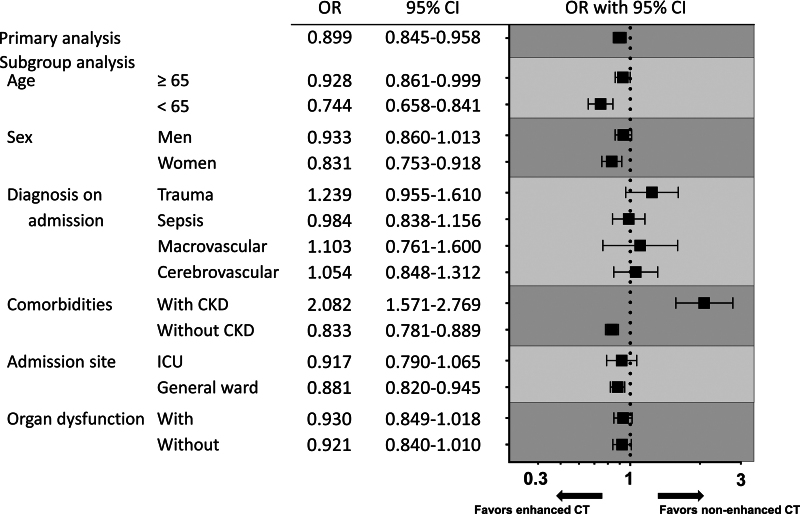
In this retrospective observational study, we examined AKI within 48 hours after CT, renal replacement therapy (RRT) dependence at discharge, and in-hospital mortality in patients undergoing contrast-enhanced CT or nonenhanced CT. We performed 1:1 propensity score matching to adjust for confounders in the association between IV contrast media use and outcomes. Subgroup analyses were performed according to age, sex, diagnosis at admission, ICU admission, and preexisting chronic kidney disease (CKD).
This study used the Medical Data Vision database between 2008 and 2019. This database is Japan's largest commercially available hospital-based claims database, covering about 45% of acute-care hospitals in Japan, and it also records laboratory results.
None.
The study included 144,149 patients with (49,057) and without (95,092) contrast media exposure, from which 43,367 propensity score-matched pairs were generated. Between the propensity score-matched groups of overall patients, exposure to contrast media showed no significant risk of AKI (4.6% vs. 5.1%; odds ratio [OR], 0.899; 95% CI, 0.845-0.958) or significant risk of RRT dependence (0.6% vs. 0.4%; OR, 1.297; 95% CI, 1.070-1.574) and significant benefit for in-hospital mortality (5.4% vs. 6.5%; OR, 0.821; 95% CI, 0.775-0.869). In subgroup analyses regarding preexisting CKD, exposure to contrast media was a significant risk for AKI in patients with CKD but not in those without CKD.
In this large-scale observational study, IV contrast media was not associated with an increased risk of AKI but concurrently showed beneficial effects on in-hospital mortality among patients requiring emergency admission.
本研究旨在阐明接受紧急入院治疗的患者中,静脉注射对比剂 CT 与急性肾损伤(AKI)和院内死亡率之间的关联。
在这项回顾性观察性研究中,我们检查了 CT 后 48 小时内的 AKI、出院时依赖肾脏替代治疗(RRT)以及接受对比增强 CT 或非增强 CT 的患者的院内死亡率。我们进行了 1:1 倾向评分匹配,以调整 IV 对比剂使用与结局之间的混杂因素。根据年龄、性别、入院诊断、入住重症监护病房(ICU)和预先存在的慢性肾脏病(CKD)进行亚组分析。
本研究使用了 2008 年至 2019 年期间的医疗数据视觉数据库。该数据库是日本最大的商业可用的医院索赔数据库,覆盖了日本约 45%的急性护理医院,并且还记录了实验室结果。
无。
研究纳入了 144149 例有(49057 例)和无(95092 例)对比剂暴露的患者,从中生成了 43367 对倾向评分匹配对。在总体患者的倾向评分匹配组中,对比剂暴露与 AKI(4.6%比 5.1%;比值比 [OR],0.899;95%CI,0.845-0.958)或 RRT 依赖(0.6%比 0.4%;OR,1.297;95%CI,1.070-1.574)的风险无显著关联,并且对院内死亡率有显著获益(5.4%比 6.5%;OR,0.821;95%CI,0.775-0.869)。在预先存在 CKD 的亚组分析中,对比剂暴露是 CKD 患者 AKI 的显著风险因素,但对无 CKD 的患者则不是。
在这项大规模观察性研究中,静脉注射对比剂与 AKI 风险增加无关,但在需要紧急入院的患者中,同时显示对院内死亡率有益。