Center for Reproductive Health Equity, Department of Obstetrics and Gynecology, Oregon Health & Science University, Portland.
Center for Health Systems Effectiveness, Oregon Health & Science University, Portland.
JAMA Health Forum. 2024 Aug 2;5(8):e242755. doi: 10.1001/jamahealthforum.2024.2755.
Nineteen states have passed legislation requiring insurers to cover the dispensation of a 12-month supply of short-acting, hormonal contraception.
To determine whether 12-month contraceptive supply policies were associated with an increase in the receipt of 12-month or longer supply of contraception.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study included data from all female Medicaid enrollees aged 18 to 44 years who used short-acting hormonal contraception (ie, pill, patch, or ring) from 2016 to 2020.
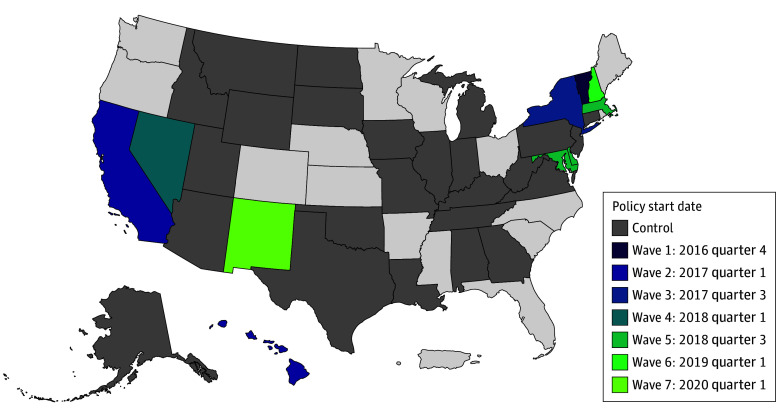
Eleven treatment states where legislation required insurers to cover a 12-month supply of contraception to continuing users and 25 comparison states without such legislation prior to December 2020.
Proportion of contraception months received via a single 12-month or longer fill.
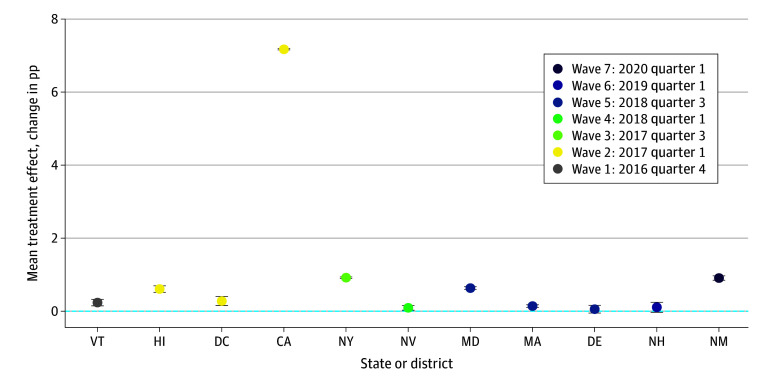
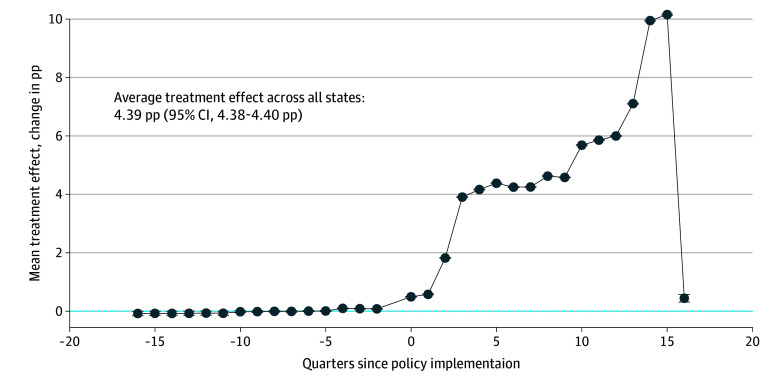
This study included 48 255 512 months of dispensed oral pill, patch, and ring contraception prescription supply among 4 778 264 female Medicaid enrollees. The majority of months of supplied contraception were for the contraceptive pill rather than the patch or ring. In a staggered difference-in-differences model, the 12-month supply policy was associated with an estimated 4.39-percentage point (pp) increase (95% CI, 4.38 pp-4.40 pp) in the proportion of contraception dispensed as part of a 12-month or longer supply, from a mean of 0.11% in treatment states during the first quarter of the study period. Investigating the heterogeneity in policy association across states, California stood out with a 7.17-pp increase (95% CI, 7.15 pp-7.19 pp) in the proportion of contraception dispensed as a 12-month or longer supply; in the other 10 treatment states, the policy association was less than 1 pp.
In this cohort study of Medicaid recipients using short-acting hormonal contraception, the passage of a 12-month contraceptive supply policy was associated with a minimal increase in the proportion of contraception dispensed through a 12-month or longer supply.
19 个州已经通过立法,要求保险公司为短期、激素避孕药物的 12 个月供应量提供保障。
确定 12 个月避孕药供应政策是否与增加 12 个月或更长时间的避孕药供应有关。
设计、环境和参与者:这项回顾性队列研究包括了所有 18 至 44 岁的女性医疗补助参保者的数据,这些参保者在 2016 年至 2020 年期间使用了短期激素避孕药(即药丸、贴片或环)。
11 个治疗州的立法要求保险公司为连续使用者提供 12 个月的避孕药供应,而在 2020 年 12 月之前,25 个对照州没有这样的立法。
通过单次 12 个月或更长时间的配药获得的避孕药供应月数的比例。
这项研究包括了 48255512 个月的口服避孕药、贴片和环的处方供应,涉及 4778264 名女性医疗补助参保者。供应的避孕药月数主要是避孕药,而不是贴片或环。在交错的差异-差异分析模型中,12 个月的供应政策与作为 12 个月或更长时间供应的一部分的避孕药配药比例估计增加了 4.39 个百分点(95%CI,4.38 个百分点-4.40 个百分点),从研究期间第一季度治疗州的平均 0.11%。调查各州政策关联的异质性时,加利福尼亚州的表现尤为突出,12 个月或更长时间供应的避孕药配药比例增加了 7.17 个百分点(95%CI,7.15 个百分点-7.19 个百分点);在其他 10 个治疗州,政策关联不到 1 个百分点。
在这项使用短期激素避孕药的医疗补助受助人的队列研究中,通过 12 个月避孕药供应政策的通过与通过 12 个月或更长时间的供应配药的避孕药比例的微小增加有关。