Institute of Cardiovascular Sciences, University of Birmingham, Medical School, Vincent Drive, Birmingham B15 2TT, UK.
West Midlands NHS Secure Data Environment, University Hospitals Birmingham NHS Foundation Trust, Mindelsohn Way, Birmingham B15 2TH, UK.
Eur Heart J. 2024 Sep 29;45(36):3707-3717. doi: 10.1093/eurheartj/ehae539.
The role of gender in decision-making for oral anticoagulation in patients with atrial fibrillation (AF) remains controversial.
The population cohort study used electronic healthcare records of 16 587 749 patients from UK primary care (2005-2020). Primary (composite of all-cause mortality, ischaemic stroke, or arterial thromboembolism) and secondary outcomes were analysed using Cox hazard ratios (HR), adjusted for age, socioeconomic status, and comorbidities.
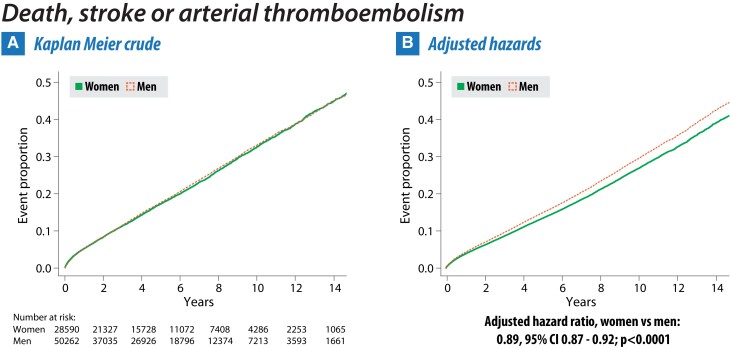
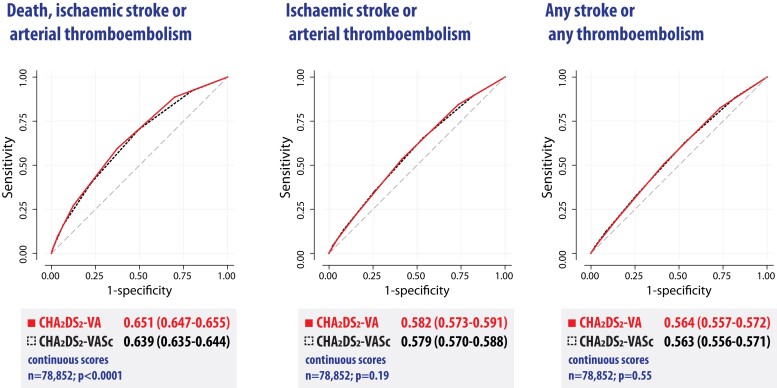
78 852 patients were included with AF, aged 40-75 years, no prior stroke, and no prescription of oral anticoagulants. 28 590 (36.3%) were women, and 50 262 (63.7%) men. Median age was 65.7 years (interquartile range 58.5-70.9), with women being older and having other differences in comorbidities. During a total follow-up of 431 086 patient-years, women had a lower adjusted primary outcome rate with HR 0.89 vs. men (95% confidence interval [CI] 0.87-0.92; P < .001) and HR 0.87 after censoring for oral anticoagulation (95% CI 0.83-0.91; P < .001). This was driven by lower mortality in women (HR 0.86, 95% CI 0.83-0.89; P < .001). No difference was identified between women and men for the secondary outcomes of ischaemic stroke or arterial thromboembolism (adjusted HR 1.00, 95% CI 0.94-1.07; P = .87), any stroke or any thromboembolism (adjusted HR 1.02, 95% CI 0.96-1.07; P = .58), and incident vascular dementia (adjusted HR 1.13, 95% CI 0.97-1.32; P = .11). Clinical risk scores were only modest predictors of outcomes, with CHA2DS2-VA (ignoring gender) superior to CHA2DS2-VASc for primary outcomes in this population (receiver operating characteristic curve area 0.651 vs. 0.639; P < .001) and no interaction with gender (P = .45).
Removal of gender from clinical risk scoring could simplify the approach to which patients with AF should be offered oral anticoagulation.
性别在房颤(AF)患者口服抗凝治疗决策中的作用仍存在争议。
本人群队列研究使用了来自英国初级保健的 16587749 名患者的电子医疗记录(2005-2020 年)。使用 Cox 风险比(HR)分析主要(全因死亡率、缺血性卒中和动脉血栓栓塞的复合结局)和次要结局,调整年龄、社会经济地位和合并症。
共纳入 78852 例有 AF、年龄 40-75 岁、无既往卒中且未开具口服抗凝药物的患者。其中 28590 例(36.3%)为女性,50262 例(63.7%)为男性。中位年龄为 65.7 岁(四分位距 58.5-70.9),女性年龄较大且合并症存在其他差异。在总计 431086 患者年的随访中,女性的调整后主要结局发生率较低,HR 为 0.89(95%置信区间 [CI] 0.87-0.92;P <.001),且在口服抗凝药物后进行 censoring 时 HR 为 0.87(95% CI 0.83-0.91;P <.001)。这主要是由于女性的死亡率较低(HR 0.86,95% CI 0.83-0.89;P <.001)。女性与男性在缺血性卒中和动脉血栓栓塞的次要结局(调整后 HR 1.00,95% CI 0.94-1.07;P =.87)、任何卒中和任何血栓栓塞(调整后 HR 1.02,95% CI 0.96-1.07;P =.58)以及新发血管性痴呆(调整后 HR 1.13,95% CI 0.97-1.32;P =.11)方面无差异。临床风险评分仅对结局有适度的预测作用,在该人群中,CHA2DS2-VA(忽略性别)优于 CHA2DS2-VASc 预测主要结局(接受者操作特征曲线下面积 0.651 比 0.639;P <.001),且与性别无交互作用(P =.45)。
从临床风险评分中去除性别可能会简化 AF 患者应接受口服抗凝治疗的方法。