Russo Chiara, Mikulska Malgorzata, Delfino Emanuele, Toscanini Federica, Mezzogori Laura, Schiavoni Riccardo, Bartalucci Claudia, Angelucci Emanuele, Bartalucci Giulia, Gambella Massimiliano, Raiola Anna Maria, Morici Paola, Crea Francesca, Chiola Silvia, Morbelli Silvia Daniela, Marchese Anna, Bassetti Matteo
Division of Infectious Diseases, Department of Health Sciences (DISSAL), University of Genoa, Genoa, Italy.
Infectious Diseases Unit, IRCCS Ospedale Policlinico San Martino, L.Go R. Benzi, 10, 16132, Genoa, Italy.
Infect Dis Ther. 2024 Oct;13(10):2179-2193. doi: 10.1007/s40121-024-01035-9. Epub 2024 Sep 4.
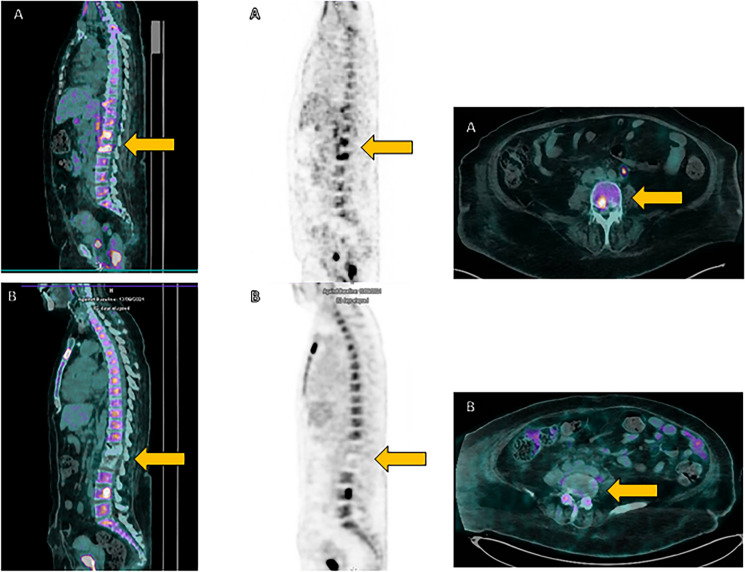
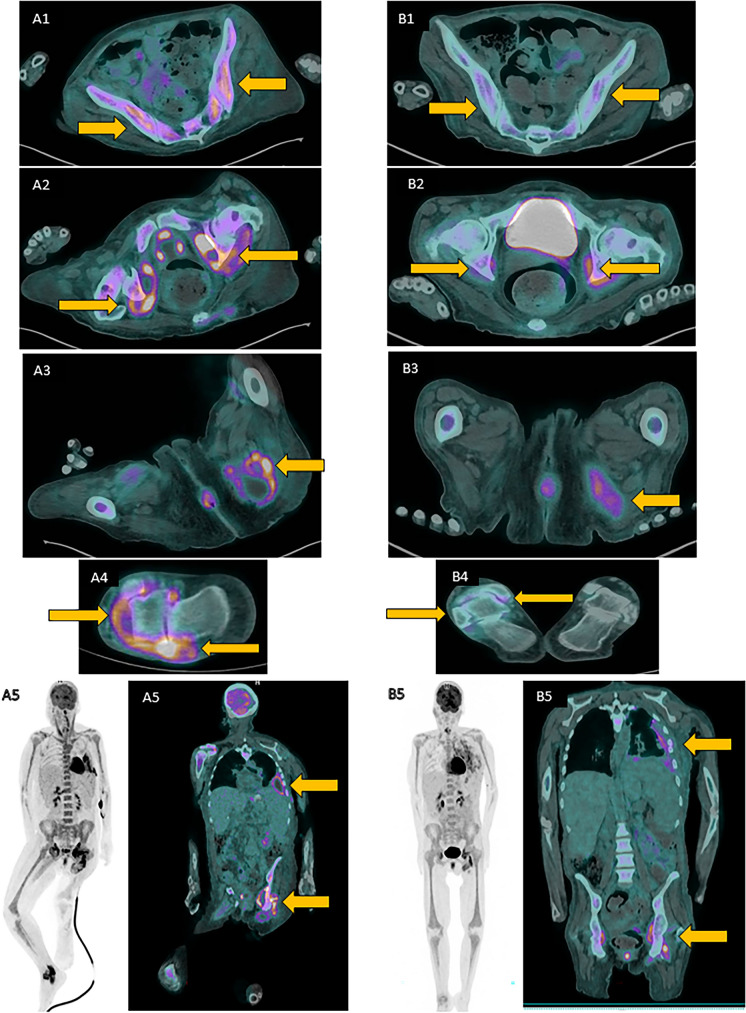
Mycoplasma hominis can be a part of human urogenital tract microbiome, and it is a frequent cause of urogenital infections. In rare cases, it can also cause extragenital infections, especially in immunocompromised patients. In this case series, we report two cases and provide a literature review of extragenital infections caused by M. hominis in patients with hypogammaglobulinemia. Patient 1 was a 61-year-old woman with diffuse large B-cell lymphoma who, after rituximab-containing chemotherapy and CAR-T therapy, developed M. hominis spondylodiscitis. Patient 2 was a 50-year-old woman with congenital hypogammaglobulinemia who developed disseminated M. hominis infection involving pleura, muscles, and right ankle. Antibiotic therapy with levofloxacin and doxycycline for 10 weeks in patient 1 and with levofloxacin alone for 6 weeks in patient 2 led to infection resolution. The literature review identified 14 additional cases reporting M. hominis extragenital infection in patients with hypogammaglobulinemia. M. hominis should also be suspected as an etiological agent of extragenital infection in patients with B-cell immunodeficiency with a clinical picture of persistent, standard-culture negative infection, particularly with arthritis or abscess formation. Even if M. hominis can grow on standard bacterial medium, in suspected cases molecular methods should be promptly used for correct diagnostic work-up and successful therapy.
人型支原体可成为人类泌尿生殖道微生物群的一部分,是泌尿生殖道感染的常见病因。在罕见情况下,它也可引起泌尿生殖道以外的感染,尤其是在免疫功能低下的患者中。在本病例系列中,我们报告了两例病例,并对低丙种球蛋白血症患者中人型支原体引起的泌尿生殖道以外感染进行了文献综述。病例1是一名61岁患有弥漫性大B细胞淋巴瘤的女性,在接受含利妥昔单抗的化疗和CAR-T治疗后,发生了人型支原体性脊椎椎间盘炎。病例2是一名50岁患有先天性低丙种球蛋白血症的女性,发生了播散性人型支原体感染,累及胸膜、肌肉和右踝。病例1使用左氧氟沙星和多西环素进行10周的抗生素治疗,病例2仅使用左氧氟沙星进行6周的治疗,感染均得到缓解。文献综述还发现了另外14例报告低丙种球蛋白血症患者中人型支原体泌尿生殖道以外感染的病例。对于有持续的、标准培养阴性感染临床表现的B细胞免疫缺陷患者,尤其是伴有关节炎或脓肿形成的患者,也应怀疑人型支原体是泌尿生殖道以外感染的病原体。即使人型支原体可在标准细菌培养基上生长,但在疑似病例中,应及时采用分子方法进行正确的诊断检查和成功治疗。