Department of Epidemiology, Gillings School of Global Public Health, University of North Carolina, Chapel Hill.
Injury Prevention Research Center, University of North Carolina, Chapel Hill.
JAMA Netw Open. 2024 Sep 3;7(9):e2429454. doi: 10.1001/jamanetworkopen.2024.29454.
Since 2014, Medicaid expansion has been implemented in many states across the US, increasing health care access among vulnerable populations, including formerly incarcerated people who experience higher mortality rates than the general population.
To examine population-level association of Medicaid expansion with postrelease mortality from all causes, unintentional drug overdoses, opioid overdoses, polydrug overdoses, suicides, and homicides among formerly incarcerated people in Rhode Island (RI), which expanded Medicaid, compared with North Carolina (NC), which did not expand Medicaid during the study period.
DESIGN, SETTING, AND PARTICIPANTS: A cohort study was conducted using incarceration release data from January 1, 2009, to December 31, 2018, linked to death records from January 1, 2009, to December 31, 2019, on individuals released from incarceration in RI and NC. Data analysis was performed from August 20, 2022, to February 15, 2024. Participants included those aged 18 years or older who were released from incarceration. Individuals who were temporarily held during ongoing judicial proceedings, died during incarceration, or not released from incarceration during the study period were excluded.
Full Medicaid expansion in RI effective January 1, 2014.
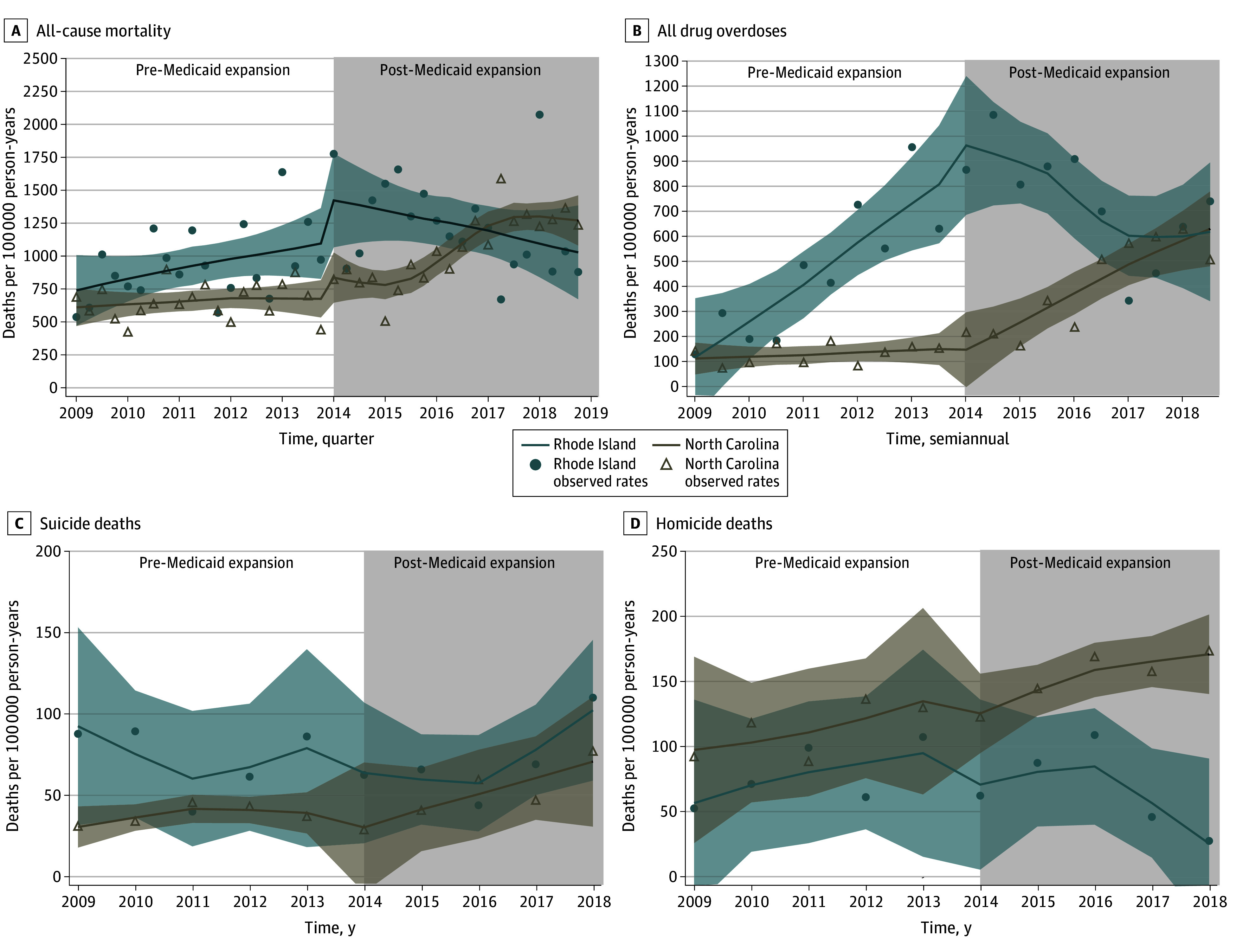
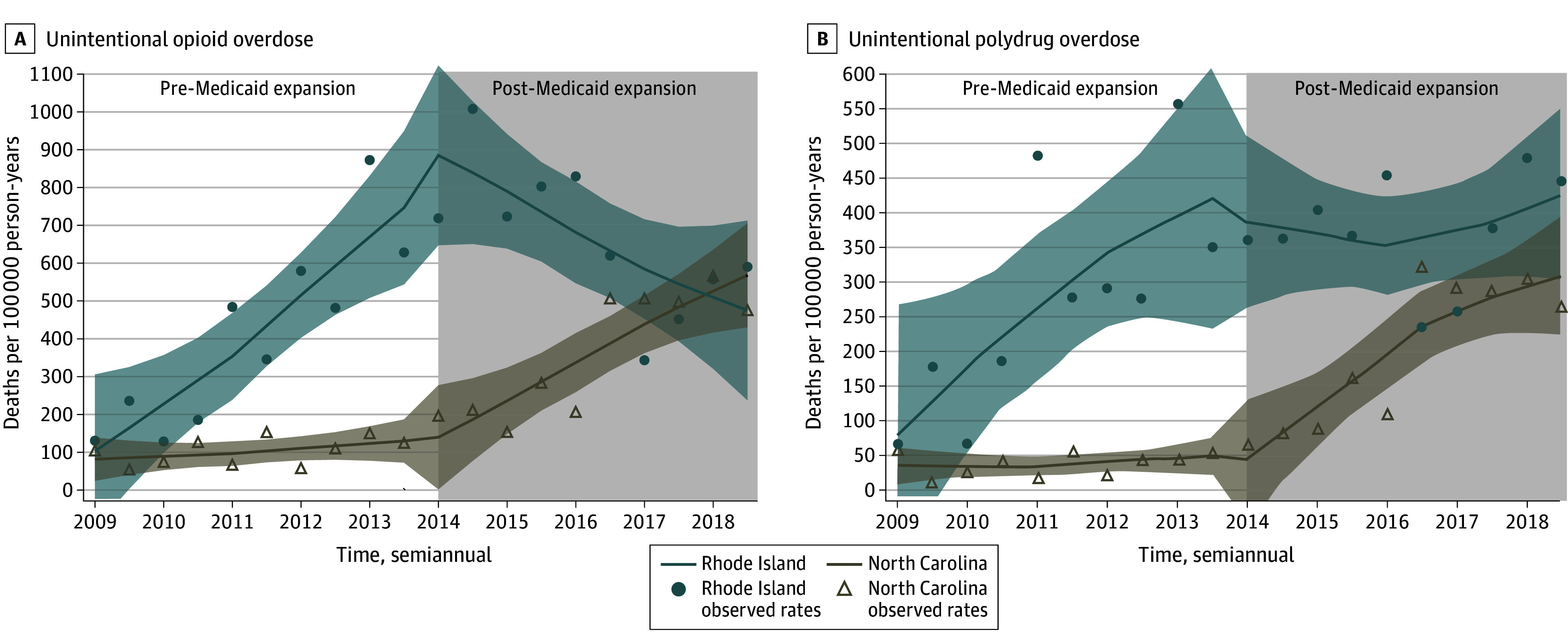
Mortality from all causes, unintentional drug overdoses, unintentional opioid and polydrug overdoses, suicides, and homicides.
Between 2009 and 2018, 17 824 individuals were released from RI prisons (mean [SD] age, 38.39 [10.85] years; 31 512 [89.1%] male) and 160 861 were released from NC prisons (mean [SD] age, 38.28 [10.84] years; 209 021 [87.5%] male). Compared with NC, people who were formerly incarcerated in RI experienced a sustained decrease of 72 per 100 000 person-years (95% CI, -108 to -36 per 100 000 person-years) in all-cause mortality per quarter after Medicaid expansion. Similar decreases were observed in RI in drug overdose deaths (-172 per 100 000 person-years per 6 months; 95% CI, -226 to -117 per 100 000 person-years), including opioid and polydrug overdoses, and homicide deaths (-23 per 100 000 person-years per year; 95% CI, -50 to 4 per 100 000 person-years) after Medicaid expansion. Suicide mortality did not change after Medicaid expansion. After Medicaid expansion in RI, non-Hispanic White individuals experienced 3 times greater sustained decreases in all-cause mortality than all racially minoritized individuals combined, while non-Hispanic Black individuals did not experience any substantial benefits. There was no modification by sex. Individuals aged 30 years or older experienced greater all-cause mortality reduction after Medicaid expansion than those younger than 30 years.
Medicaid expansion in RI was associated with a decrease in all-cause, overdose, and homicide mortality among formerly incarcerated people. However, these decreases were most observed among White individuals, while racially minoritized individuals received little to no benefits in the studied outcomes.
重要性:自 2014 年以来,美国许多州都实施了医疗补助扩大计划,增加了弱势群体的医疗保健机会,包括以前被监禁的人,他们的死亡率高于一般人群。
目的:研究人口水平上的关联,即在罗得岛州(RI)实施医疗补助扩大计划后,与北卡罗来纳州(NC)相比,以前被监禁的人在释放后的全因死亡率、非故意药物过量、阿片类药物过量、多药物过量、自杀和杀人率之间的关联。在研究期间,NC 没有扩大医疗补助。
设计、地点和参与者:这是一项队列研究,使用了 2009 年 1 月 1 日至 2018 年 12 月 31 日的监禁释放数据,与 2009 年 1 月 1 日至 2019 年 12 月 31 日的死亡记录相关联,研究对象是从 RI 和 NC 释放的被监禁者。数据分析于 2022 年 8 月 20 日至 2024 年 2 月 15 日进行。参与者包括年龄在 18 岁或以上、从监禁中释放的人。在此期间,暂时被关押在正在进行的司法程序中、在监禁期间死亡或未被释放的人被排除在外。
暴露:RI 于 2014 年 1 月 1 日全面扩大医疗补助。
主要结果和措施:所有原因、非故意药物过量、非故意阿片类药物和多药物过量、自杀和杀人的死亡率。
结果:2009 年至 2018 年期间,有 17824 人从 RI 监狱获释(平均[标准差]年龄为 38.39[10.85]岁;31512[89.1%]为男性),有 160861 人从 NC 监狱获释(平均[标准差]年龄为 38.28[10.84]岁;209021[87.5%]为男性)。与 NC 相比,RI 以前被监禁的人在医疗补助扩大后的每季度全因死亡率持续下降 72 人/10 万人(95%CI,-108 至-36 人/10 万人)。在 RI,类似的下降也发生在药物过量死亡(每 6 个月减少 172 人/10 万人;95%CI,-226 至-117 人/10 万人),包括阿片类药物和多药物过量,以及医疗补助扩大后的杀人死亡(每年减少 23 人/10 万人;95%CI,-50 至-4 人/10 万人)。医疗补助扩大后,自杀死亡率没有变化。在 RI 实施医疗补助扩大后,非西班牙裔白人个体的全因死亡率持续下降幅度是所有种族少数群体个体的 3 倍,而非西班牙裔黑人个体则没有获得任何实质性的好处。性别没有影响。30 岁或以上的个体在医疗补助扩大后全因死亡率的降低幅度大于 30 岁以下的个体。
结论和相关性:RI 的医疗补助扩大与以前被监禁的人的全因、过量和杀人死亡率下降有关。然而,这些下降主要发生在白人个体中,而种族少数群体在研究结果中几乎没有受益。