Giri Shamik, Ahmed Ahmed A, Zeid Mohamed, Khan Muhammad S, Giri Subhasis K
Medicine, St. James's Hospital and Trinity College Dublin, Dublin, IRL.
Urology, University Hospital Limerick, Limerick, IRL.
Cureus. 2024 Sep 19;16(9):e69749. doi: 10.7759/cureus.69749. eCollection 2024 Sep.
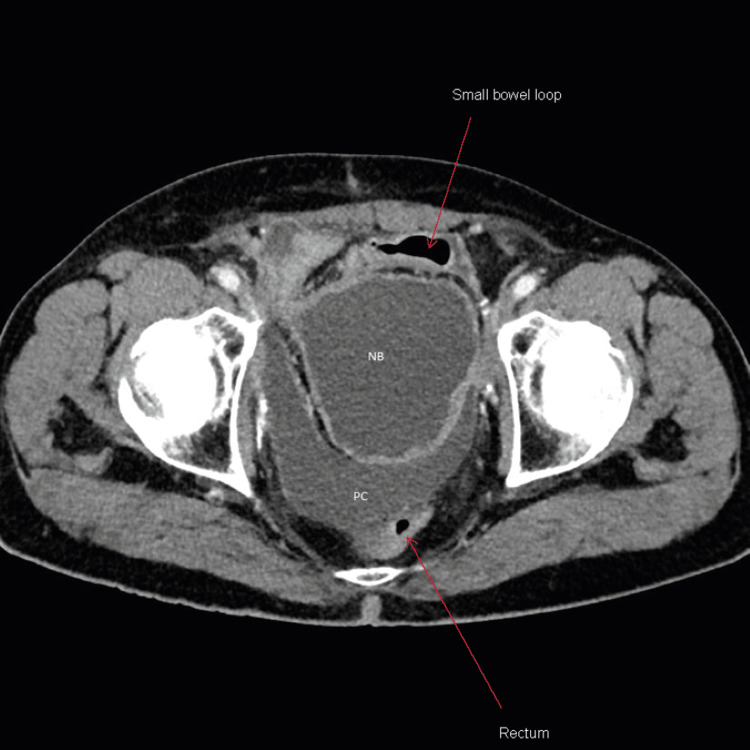
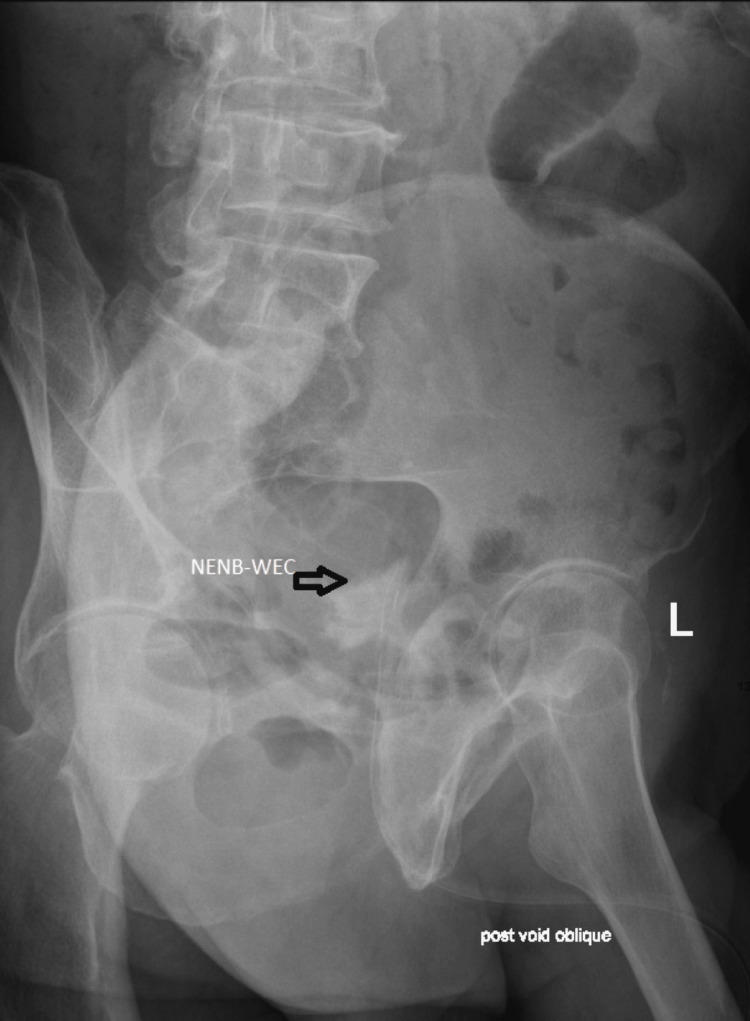
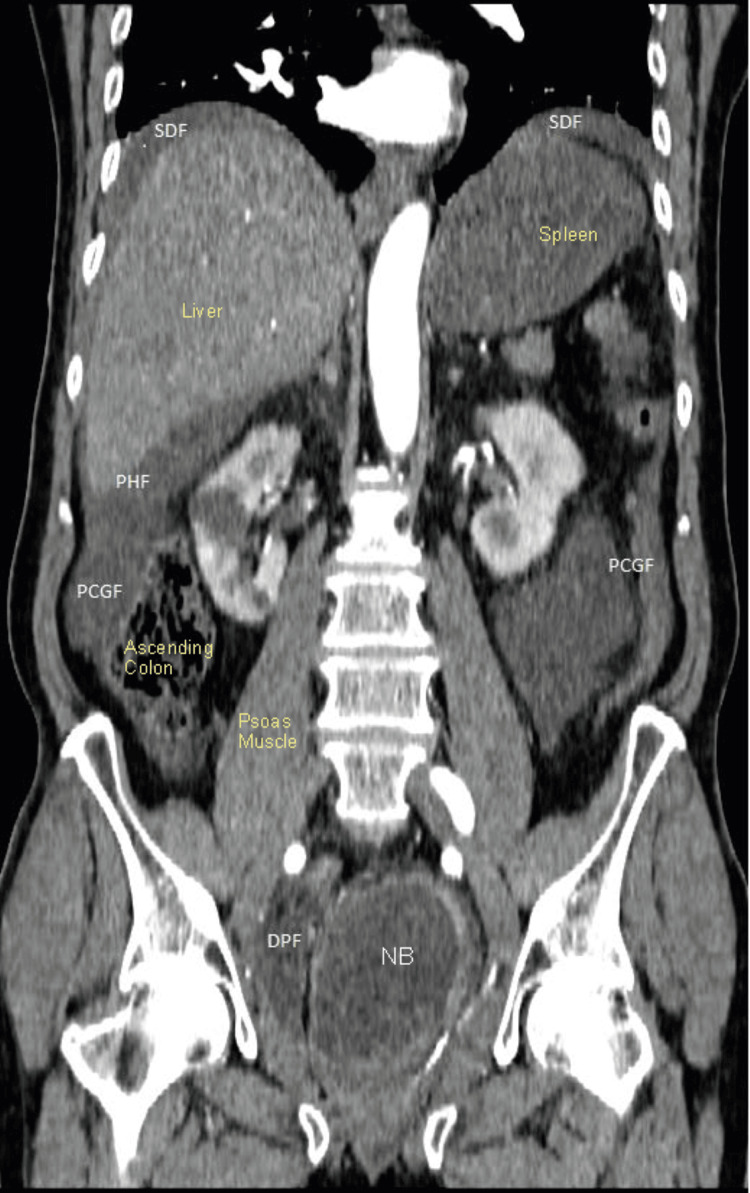
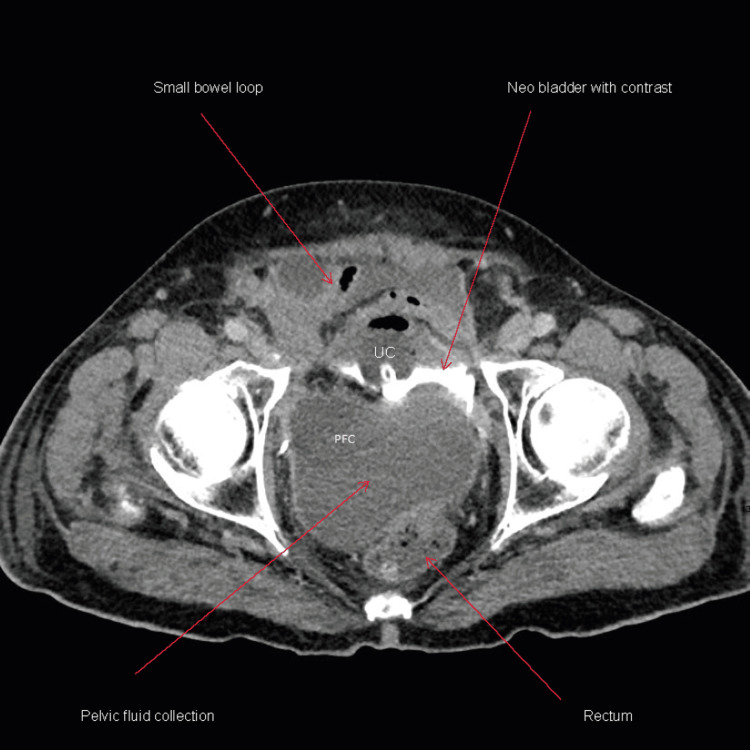
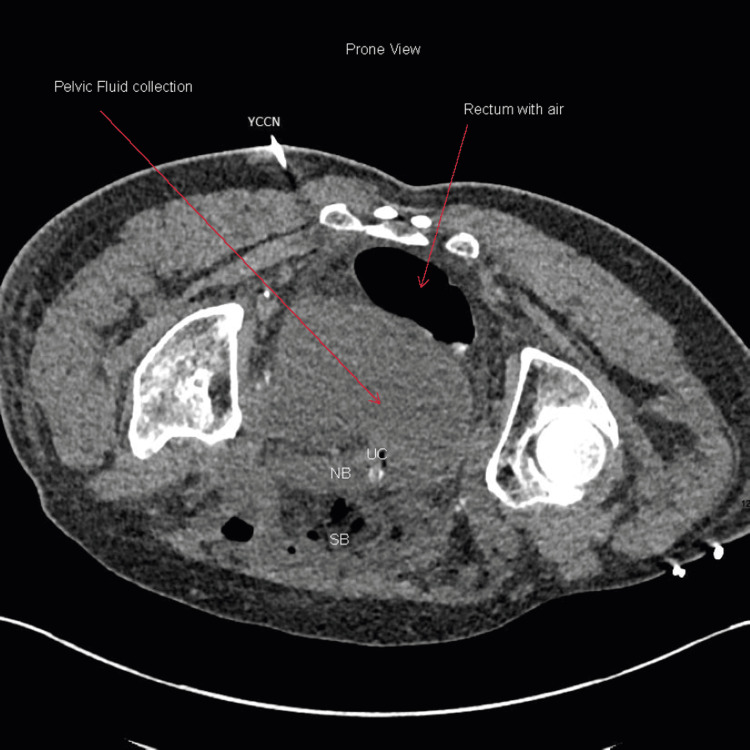
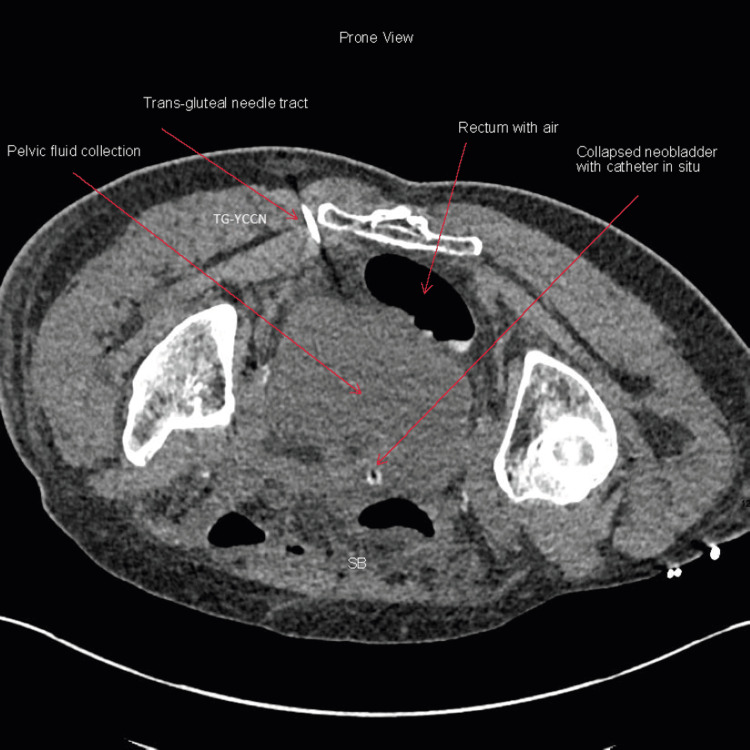
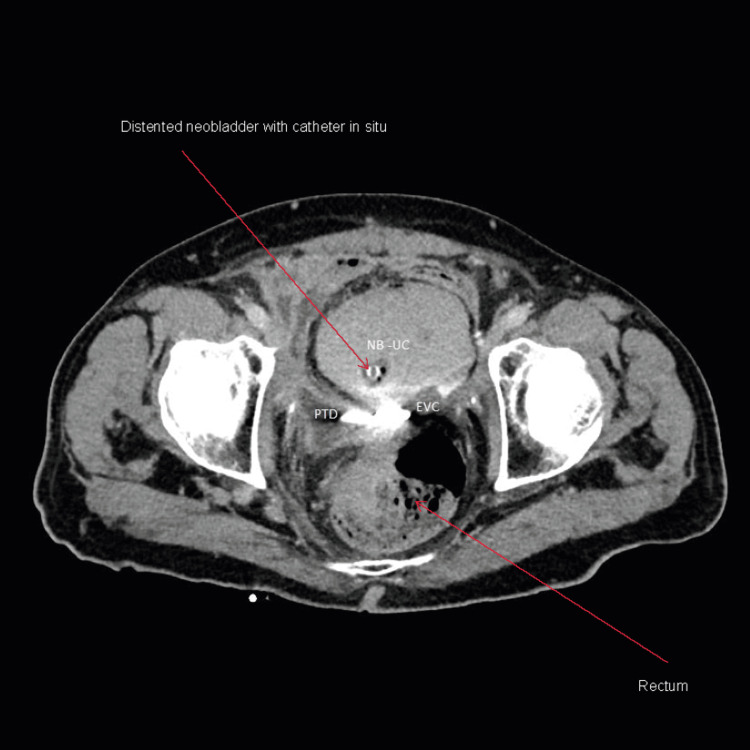
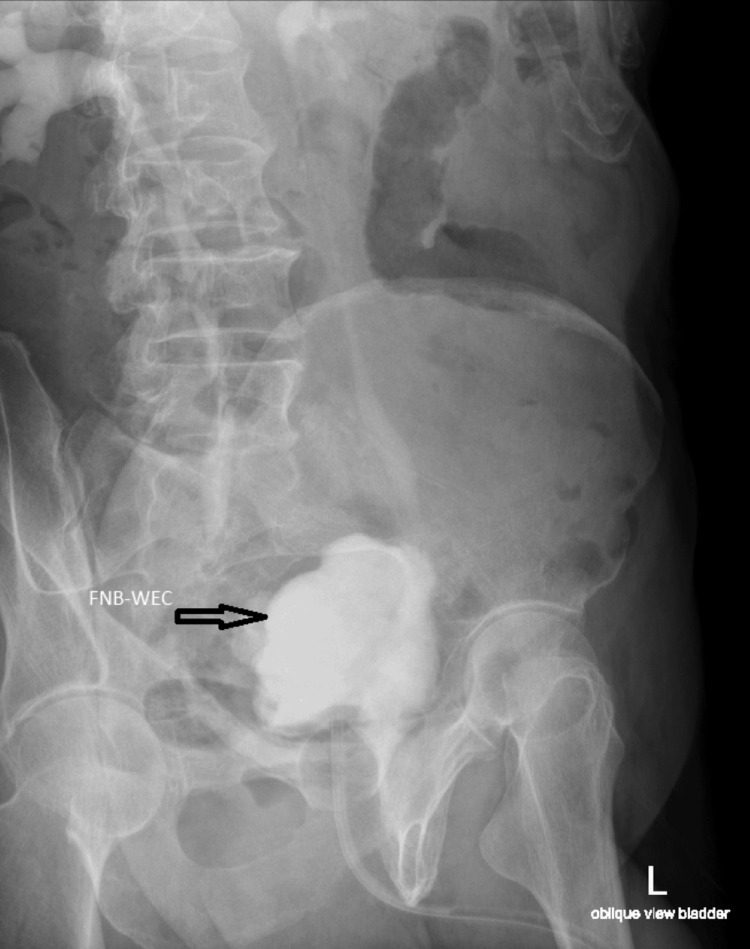
The orthotopic ileal neobladder is becoming a popular technique of urinary diversion after radical cystectomy (RC) for localized muscle-invasive bladder cancer (MIBC), allowing patient continence, with a more desirable body image and good quality of life. Minimally invasive robot-assisted RC and neobladder have the potential to minimize physical and psychological trauma and are increasingly being adopted for patients with MIBC worldwide. Spontaneous perforation of orthotopic neobladder is uncommon;however, it represents serious complications. Solitary binge drinking can be dangerous in a patient with a neobladder because of reduced level of consciousness and overdistension of the neobladder. We report a case of spontaneous ileal neobladder perforations one year post-robotic RC secondary to blackouts from binge drinking. We also describe nonoperative active management and review the literature. A 66-year-old gentleman was brought by ambulance to our emergency department with a reduced level of consciousness, vomiting, and abdominal pain in the early hours of the morning. Collateral history revealed that he had drunk alcohol alone the night before at his home where he lives alone. Initial examination revealed tachycardia and hypotension. Immediate resuscitation using the sepsis six protocol included intravenous normal saline, blood culture, broad-spectrum antibiotic, lactate measurement, and insertion of a urethral catheter to monitor urine output. Following contrast-enhanced computed tomography (CECT) of the abdomen and pelvis, the patient was referred to a urologist. A diagnosis of spontaneous perforation of the neobladder was made. A nonoperative or 'conservative' management approach was adopted with careful active monitoring at the intensive care unit (ICU) involving a multidisciplinary team. Follow-up CT was performed to assess radiological recovery. The patient recovered successfully and was discharged home five weeks post-admission with an indwelling urethral catheter. The catheter was removed 10 weeks post-admission following a cystogram confirming the integrity of the neobladder. The patient has preserved neobladder function and continence and is doing well until the last follow-up at six months post-discharge. Patients with neobladder should be rigorously counseled about the importance of timed voiding, intermittent self-catheter, serious consequences of solitary binge drinking, and urinary retention.
原位回肠新膀胱术正成为局部肌层浸润性膀胱癌(MIBC)根治性膀胱切除术(RC)后一种常用的尿流改道术,能让患者实现控尿,拥有更理想的身体形象和良好的生活质量。微创机器人辅助RC和新膀胱术有潜力将身体和心理创伤降至最低,在全球范围内越来越多地被用于MIBC患者。原位新膀胱自发性穿孔并不常见,但其是严重的并发症。对于新膀胱患者,单次大量饮酒可能很危险,因为意识水平降低和新膀胱过度扩张。我们报告一例机器人辅助RC术后一年因大量饮酒致昏厥继发回肠新膀胱自发性穿孔的病例。我们还描述了非手术积极治疗方法并回顾了相关文献。一名66岁男性清晨被救护车送至我院急诊科,意识水平降低、呕吐且腹痛。旁系病史显示他前一晚独自在家饮酒。初步检查发现心动过速和低血压。立即按照脓毒症六步法进行复苏,包括静脉输注生理盐水、血培养、使用广谱抗生素、测量乳酸水平以及插入尿道导管以监测尿量。在进行腹部和盆腔增强CT(CECT)后,患者被转诊至泌尿科医生处。诊断为新膀胱自发性穿孔。采用非手术或“保守”治疗方法,在重症监护病房(ICU)由多学科团队进行仔细的积极监测。进行后续CT检查以评估影像学恢复情况。患者成功康复,入院五周后带留置尿道导管出院。入院十周后,膀胱造影证实新膀胱完整,随后拔除导管。患者保留了新膀胱功能和控尿能力,出院后六个月最后一次随访时情况良好。应严格告知新膀胱患者定时排尿、间歇性自我导尿的重要性、单次大量饮酒的严重后果以及尿潴留问题。