Hagenimana Jean Pierre, Banguti Paulin Ruhato, Anderson Rebecca Lynn Churchill, Tuyishime Jean de Dieu, Nyirigira Gaston, Tuyishime Eugene
Department of Anesthesia and Critical Care, Bushenge Provincial Hospital, Rwanda.
Department of Anesthesia, Critical Care and Emergency Medicine, University of Rwanda.
Afr J Emerg Med. 2024 Dec;14(4):258-262. doi: 10.1016/j.afjem.2024.08.009. Epub 2024 Sep 11.
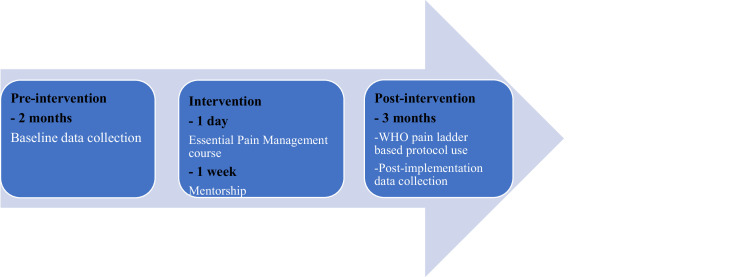
Little is known regarding the effectiveness of pain protocols and guideline use in Emergency Departments (ED) in Sub-Saharan Africa. Therefore, to shed light on this research gap, this study had the following objectives: 1) to evaluate if the implementation of the Essential Pain Management (EPM) course combined with mentorship to use the World Health Organization (WHO) pain ladder-based protocol improves the quality of pain management among trauma patients at the ED of two teaching hospitals in Rwanda; and 2) to determine barriers to implementing the WHO pain ladder-based protocol among trauma patients in the same settings.
This was a pre- and post-intervention study. The intervention was 1-day essential pain management training for ED clinical staff followed by 1 week mentorship on the use of the WHO pain ladder-based protocol.
We enrolled 261 patients (47.5% pre versus 52.5% post intervention), most of them were aged between 21 and 40 (60% pre versus 33% post intervention), and male (76% pre versus 73% post intervention). The quality of pain management at the ED improved as shown by the decrease of the number of patients with undocumented pain scores from 58% to 24% after the intervention (p-value > 0.001) and the increase of the number of patients with mild pain from 37% to 62% (p-value > 0.001). In addition, patients who were satisfied with the quality of pain management increased significantly from 42% before the intervention to 80% (p-value > 0.001). Barriers to the implementation of the WHO pain ladder-based protocol were identified related to staff (i.e. inadequate experience), to the hospital (i.e. poor documentation), and to patients (i.e. reluctance to report pain).
The implementation of the EPM course along with mentorship to use the WHO pain ladder-based protocol significantly improved the quality of pain management for trauma patients in EDs of both referral hospitals. Despite this, some barriers remain unfixed such as inadequate staff experience, poor documentation, and patient's reluctance to report pain. Appropriate interventions should be implemented to address the identified barriers and ensure adequate pain management for patients admitted at EDs in public hospitals in Rwanda.
关于撒哈拉以南非洲急诊科疼痛治疗方案及指南使用的有效性,人们知之甚少。因此,为填补这一研究空白,本研究有以下目标:1)评估实施基本疼痛管理(EPM)课程并结合指导以使用基于世界卫生组织(WHO)疼痛阶梯的方案,是否能提高卢旺达两家教学医院急诊科创伤患者的疼痛管理质量;2)确定在相同环境下创伤患者中实施基于WHO疼痛阶梯方案的障碍。
这是一项干预前后研究。干预措施是为急诊科临床工作人员提供为期1天的基本疼痛管理培训,随后就使用基于WHO疼痛阶梯的方案进行为期1周的指导。
我们纳入了261名患者(干预前占47.5%,干预后占52.5%),其中大多数年龄在21至40岁之间(干预前占60%,干预后占33%),且为男性(干预前占76%,干预后占73%)。急诊科疼痛管理质量有所改善,表现为干预后无疼痛评分记录的患者数量从58%降至24%(p值>0.001),轻度疼痛患者数量从37%增至62%(p值>0.001)。此外,对疼痛管理质量满意的患者从干预前的42%显著增至80%(p值>0.001)。已确定基于WHO疼痛阶梯方案实施的障碍与工作人员(即经验不足)、医院(即记录不佳)和患者(即不愿报告疼痛)有关。
实施EPM课程并结合指导以使用基于WHO疼痛阶梯的方案,显著提高了两家转诊医院急诊科创伤患者的疼痛管理质量。尽管如此,一些障碍仍未解决,如工作人员经验不足、记录不佳以及患者不愿报告疼痛。应实施适当干预措施以解决已确定的障碍,并确保卢旺达公立医院急诊科收治患者得到充分的疼痛管理。