HPB and Liver Transplant Unit, Department of General Surgery, Clinica Universidad de Navarra, University of Navarra, Pamplona, Spain.
Institute of Health Research of Navarra (IdisNA), Pamplona, Spain.
BJS Open. 2024 Sep 3;8(5). doi: 10.1093/bjsopen/zrae087.
Neoadjuvant treatment has shown promising results in patients with borderline resectable pancreatic ductal adenocarcinoma. The potential benefits of neoadjuvant treatment on long-term overall survival in patients with resectable pancreatic ductal adenocarcinoma have not yet been established. The aim of this study was to compare long-term overall survival of patients with resectable pancreatic ductal adenocarcinoma based on whether they received neoadjuvant treatment or underwent upfront surgery.
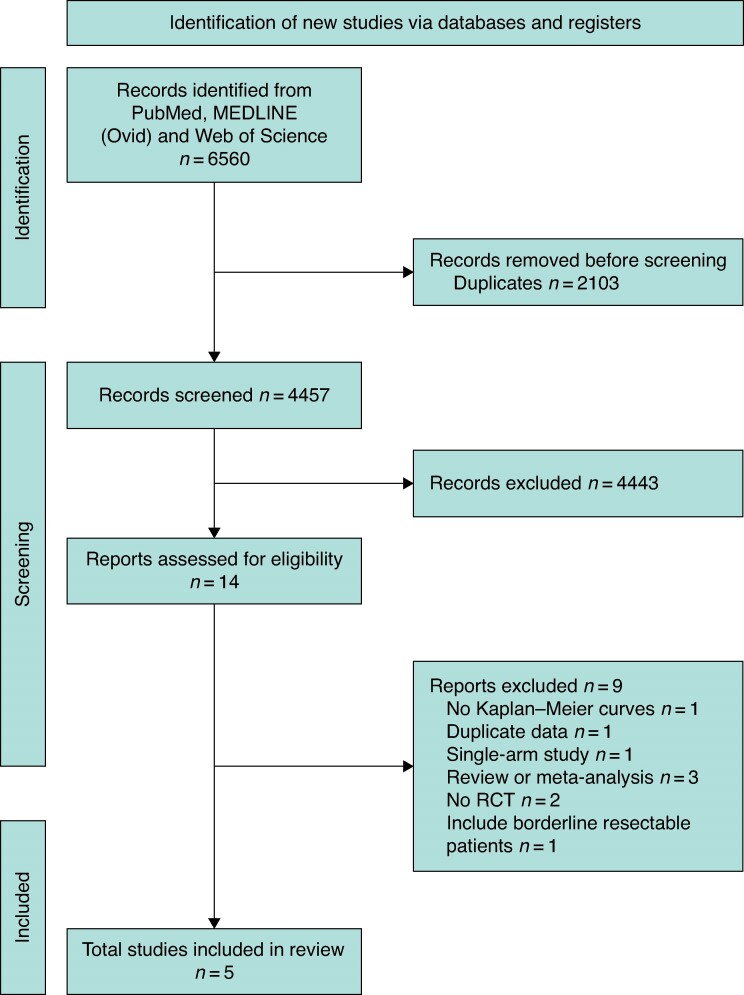
A systematic review including randomized clinical trials on the overall survival outcomes between neoadjuvant treatment and upfront surgery in patients with resectable pancreatic ductal adenocarcinoma was conducted up to 1 August 2023 from PubMed, MEDLINE and Web of Science databases. Patient-level survival data was extracted and reconstructed from available Kaplan-Meier curves. A frequentist one-stage meta-analysis was employed, using Cox-based models and a non-parametric method (restricted mean survival time), to assess the difference in overall survival between groups. A Bayesian meta-analysis was also conducted.
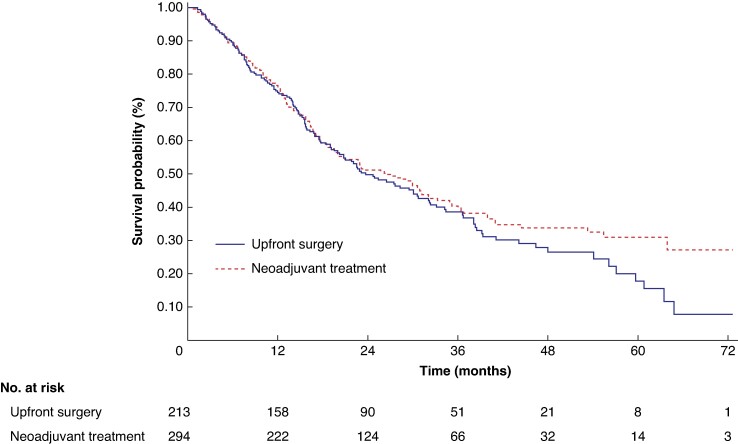
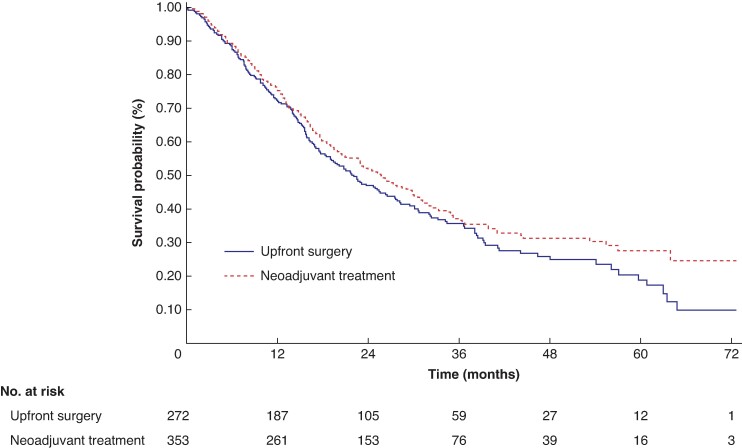
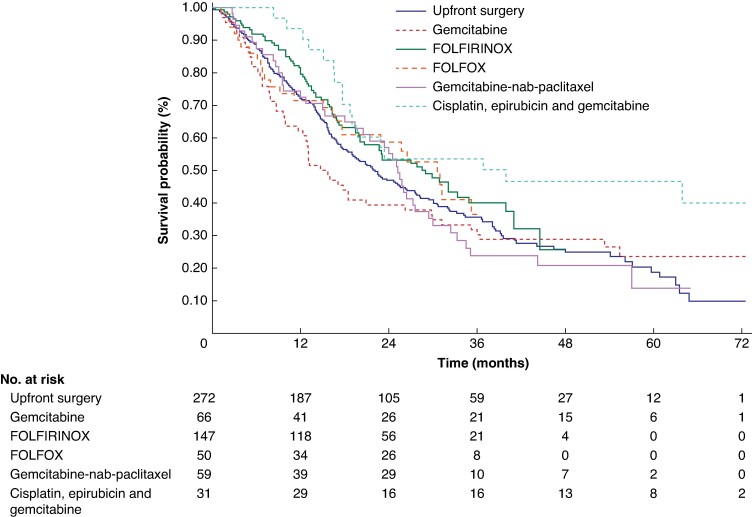
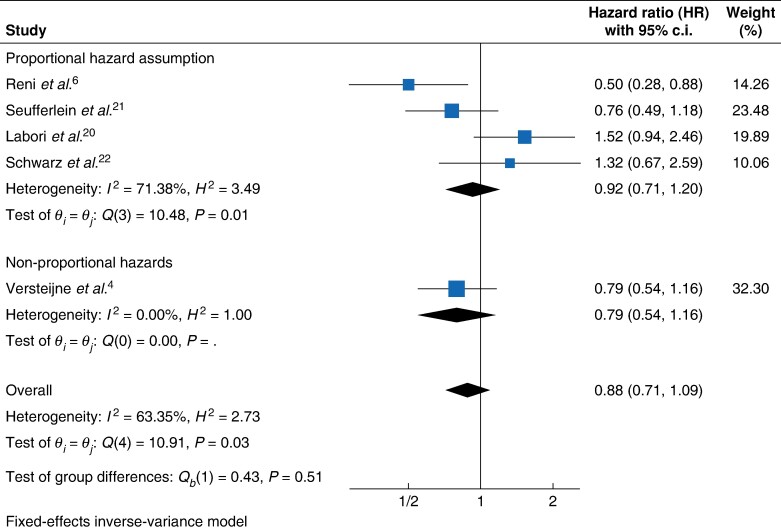
Five randomized clinical trials comprising 625 patients were included. Among patients with resectable pancreatic ductal adenocarcinoma, neoadjuvant treatment was not significantly associated with a reduction in the hazard of death compared with upfront surgery (shared frailty HR 0.88, 95% c.i. 0.72 to 1.08, P = 0.223); this result was consistent in the non-parametric restricted mean survival time model (+2.41 months, 95% c.i. -1.22 to 6.04, P < 0.194), in the sensitivity analysis that excluded randomized clinical trials with a high risk of bias (shared frailty HR 0.91 (95% c.i. 0.72 to 1.15; P = 0.424)) and in the Bayesian analysis with a posterior shared frailty HR of 0.86 (95% c.i. 0.70 to 1.05).
Neoadjuvant treatment does not demonstrate a survival advantage over upfront surgery for patients with resectable pancreatic ductal adenocarcinoma.
新辅助治疗在交界可切除的胰腺导管腺癌患者中显示出良好的效果。新辅助治疗是否能提高可切除胰腺导管腺癌患者的长期总生存率尚未确定。本研究旨在比较接受新辅助治疗和直接手术的可切除胰腺导管腺癌患者的长期总生存率。
截至 2023 年 8 月 1 日,我们从 PubMed、MEDLINE 和 Web of Science 数据库中系统地检索了新辅助治疗与直接手术治疗可切除胰腺导管腺癌患者的总生存结局的随机临床试验,并进行了综述。从可获得的 Kaplan-Meier 曲线中提取并重建了患者的生存数据。使用基于 Cox 模型和非参数方法(限制性平均生存时间)的频率论一阶段荟萃分析,评估两组之间总生存的差异。同时还进行了贝叶斯荟萃分析。
共纳入 5 项包含 625 例患者的随机临床试验。在可切除胰腺导管腺癌患者中,与直接手术相比,新辅助治疗并未显著降低死亡风险(共享脆弱性 HR 0.88,95%置信区间 0.72 至 1.08,P = 0.223);在非参数限制性平均生存时间模型中(+2.41 个月,95%置信区间 -1.22 至 6.04,P < 0.194),在排除高偏倚风险的随机临床试验的敏感性分析中(共享脆弱性 HR 0.91(95%置信区间 0.72 至 1.15;P = 0.424)),以及在贝叶斯分析中,后验共享脆弱性 HR 为 0.86(95%置信区间 0.70 至 1.05),结果均一致。
对于可切除胰腺导管腺癌患者,新辅助治疗并未显示出优于直接手术的生存优势。