Department of General, Visceral and Transplantation Surgery, Heidelberg University Hospital, Heidelberg 69120, Germany.
Section Surgical Research, University Clinic Heidelberg, Heidelberg 69120, Germany.
Function (Oxf). 2023 Mar 21;4(3):zqad011. doi: 10.1093/function/zqad011. eCollection 2023.
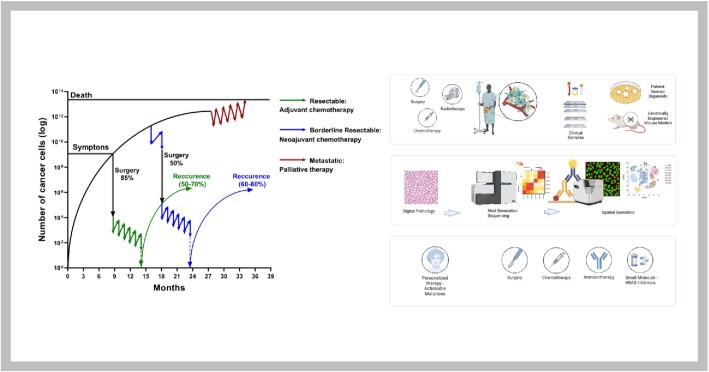
Pancreatic cancer is one of the most lethal cancers worldwide, most notably in Europe and North America. Great strides have been made in combining the most effective conventional therapies to improve survival at least in the short and medium term. The start of treatment can only be made once a diagnosis is made, which at this point, the tumor volume is already very high in the primary cancer and systemically. If caught at the earliest opportunity (in circa 20% patients) surgical resection of the primary followed by combination chemotherapy can achieve 5-year overall survival rates of 30%-50%. A delay in detection of even a few months after symptom onset will result in the tumor having only borderline resectabilty (in 20%-30% of patients), in which case the best survival is achieved by using short-course chemotherapy before tumor resection as well as adjuvant chemotherapy. Once metastases become visible (in 40%-60% of patients), cure is not possible, palliative cytotoxics only being able to prolong life by few months. Even in apparently successful therapy in resected and borderline resectable patients, the recurrence rate is very high. Considerable efforts to understand the nature of pancreatic cancer through large-scale genomics, transcriptomics, and digital profiling, combined with functional preclinical models, using genetically engineered mouse models and patient derived organoids, have identified the critical role of the tumor microenvironment in determining the nature of chemo- and immuno-resistance. This functional understanding has powered fresh and exciting approaches for the treatment of this cancer.
胰腺癌是全球最致命的癌症之一,尤其是在欧洲和北美。在将最有效的常规疗法相结合以提高短期和中期生存率方面已经取得了重大进展。只有在做出诊断后才能开始治疗,此时原发性癌症和全身性的肿瘤体积已经非常大。如果在最早的机会(约 20%的患者中)发现,可以通过手术切除原发性肿瘤并结合化疗来实现 5 年总生存率 30%-50%。即使在症状出现后仅延迟几个月进行检测,也会导致肿瘤仅具有边缘可切除性(约 20%-30%的患者),在这种情况下,在肿瘤切除前进行短期化疗以及辅助化疗可以获得最佳生存。一旦转移可见(约 40%-60%的患者),则无法治愈,姑息性细胞毒药物只能将生命延长几个月。即使在明显成功的切除和边缘可切除患者的治疗中,复发率也非常高。通过大规模基因组学、转录组学和数字分析,结合使用基因工程小鼠模型和患者来源的类器官的功能临床前模型,对胰腺癌的性质进行了大量研究,已经确定了肿瘤微环境在决定化疗和免疫耐药性方面的关键作用。这种功能上的理解为治疗这种癌症提供了新的令人兴奋的方法。