Cardiology and Cardiovascular Surgery Department, University of Medicine and Pharmacy Carol Davila, Bucharest, Romania.
Cardiology and Cardiovascular Surgery Department, University and Emergency Hospital, Bucharest, Romania.
PLoS One. 2022 May 4;17(5):e0267962. doi: 10.1371/journal.pone.0267962. eCollection 2022.
None of the conventional echocardiographic parameters alone predict increased NTproBNP level and symptoms, making diagnosis of heart failure with preserved ejection fraction (HFpEF) very difficult in some cases, in resting condition. We evaluated LA functions by 2D speckle tracking echocardiography (STE) on top of conventional parameters in HFpEF and preHF patients with diastolic dysfunction (DD), in order to establish the added value of the LA deformation parameters in the diagnosis of HFpEF.
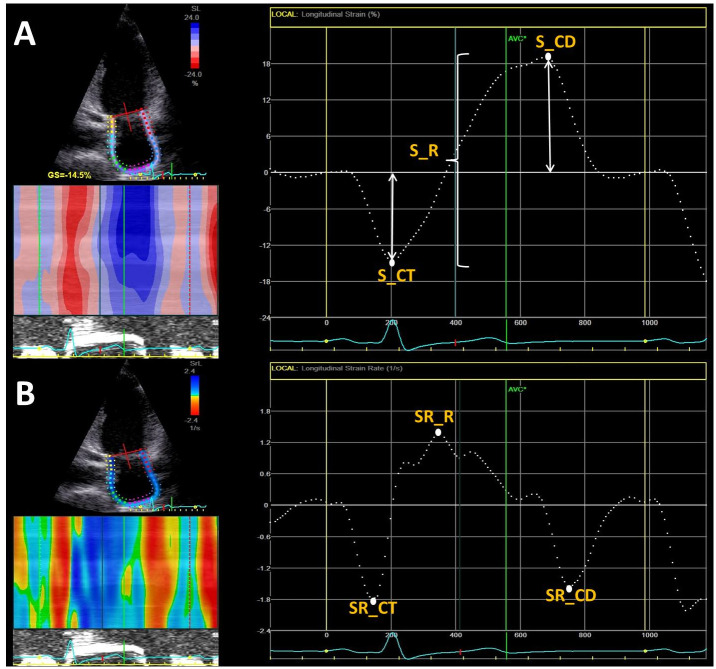
We prospectively enrolled 125 patients, 88 with HFpEF (68±9 yrs), and 37 asymptomatic with similar risk factors with DD (preHF) (61±8 yrs). We evaluated them by NTproBNP, conventional DD parameters, and STE. Global longitudinal strain (GS) was added. LA reservoir (R), conduit (C), and pump function (CT) were assessed both by volumetric and STE. 2 reservoir strain (S) derived indices were also measured, stiffness (SI) and distensibility index (DI).
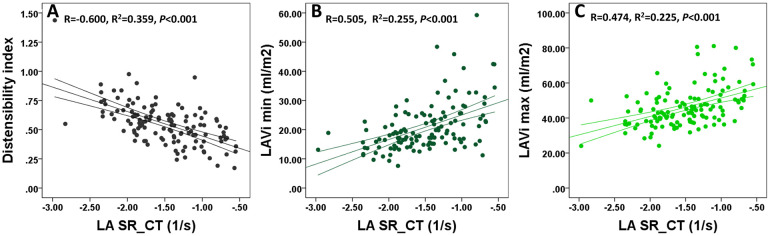
LA R and CT functions were significantly reduced in HFpEF compared to preHF group (all p<0.001), whereas conduit was similarly in both groups. SI was increased, whereas DI was reduced in HFpEF group (p<0.001). By adding LA strain analysis, from all echocardiographic parameters, SR_CT<-1.66/s and DI<0.57 (AUC = 0.76, p<0.001) demonstrated the highest accuracy to identify HFpEF diagnosis. However, by multivariate logistic regression, the model that best identifies HFpEF included only SR_CT, GS and sPAP (R2 = 0.506, p<0.001). Moreover, SR_CT, DI, and sPAP registered significant correlation with NTproBNP level.
By adding LA functional analysis, we might improve the HFpEF diagnosis accuracy, compared to present guidelines. LA pump function is the only one able to differentiates preHF from HFpEF patients at rest. A value of SR_CT < -1.66/s outperformed conventional parameters from the scoring system, reservoir strain, and LA overload indices in HFpEF diagnosis. We suggest that LA function by STE could be incorporated in the current protocol for HFpEF diagnosis at rest as a major functional criterion, in order to improve diagnostic algorithm, and also in the follow-up of patients with risk factors and DD, as a prognostic marker. Future studies are needed to validate our findings.
在静息状态下,没有任何常规超声心动图参数可以单独预测 NTproBNP 水平和症状的增加,这使得射血分数保留的心力衰竭(HFpEF)的诊断变得非常困难。我们通过二维斑点追踪超声心动图(STE)评估左心房(LA)功能,在有舒张功能障碍(DD)的 HFpEF 和 preHF 患者中加入常规参数,以确定 LA 变形参数在 HFpEF 诊断中的附加价值。
我们前瞻性纳入 125 名患者,88 名 HFpEF(68±9 岁),37 名无症状但有类似危险因素和 DD(preHF)(61±8 岁)。我们通过 NTproBNP、常规 DD 参数和 STE 评估他们。加入了整体纵向应变(GS)。通过容积和 STE 评估 LA 储备(R)、管道(C)和泵功能(CT)。还测量了 2 个储备应变(S)衍生指数,僵硬度(SI)和顺应性指数(DI)。
与 preHF 组相比,HFpEF 患者的 LA R 和 CT 功能明显降低(均 p<0.001),而两组的管道功能相似。HFpEF 组的 SI 增加,而 DI 降低(p<0.001)。通过添加 LA 应变分析,从所有超声心动图参数中,SR_CT<-1.66/s 和 DI<0.57(AUC=0.76,p<0.001)显示出最高的准确性来识别 HFpEF 诊断。然而,通过多元逻辑回归,最佳识别 HFpEF 的模型仅包括 SR_CT、GS 和 sPAP(R2=0.506,p<0.001)。此外,SR_CT、DI 和 sPAP 与 NTproBNP 水平显著相关。
通过添加 LA 功能分析,与现有指南相比,我们可能会提高 HFpEF 的诊断准确性。LA 泵功能是唯一能够区分静息状态下 preHF 和 HFpEF 患者的功能。SR_CT 的值<-1.66/s 优于评分系统、储备应变和 LA 过载指数的常规参数,在 HFpEF 诊断中具有更高的诊断价值。我们建议,STE 评估的 LA 功能可以作为主要的功能标准纳入 HFpEF 的常规诊断方案中,以改善诊断算法,也可以纳入有危险因素和 DD 的患者的随访中,作为预后标志物。需要进一步的研究来验证我们的发现。