Division of Neonatology, NHO Okayama Medical Center, 1711-1 Tamasu, Kita-ku, Okayama, 701-1192, Japan.
Department of Epidemiology, Okayama University Graduate School of Medicine, Dentistry, and Pharmaceutical Sciences, Okayama, Japan.
BMC Pediatr. 2024 Sep 30;24(1):618. doi: 10.1186/s12887-024-05090-6.
Previous research has suggested a correlation between postnatal maximum weight loss (MWL) and both neonatal mortality and morbidities in extremely preterm infants. However, the relationship between MWL and neurodevelopmental outcomes remains underexplored.
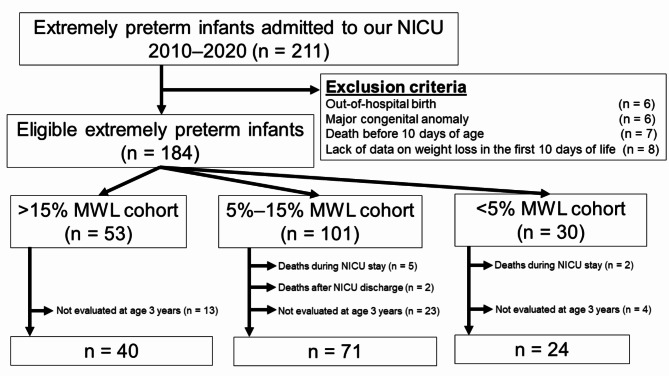
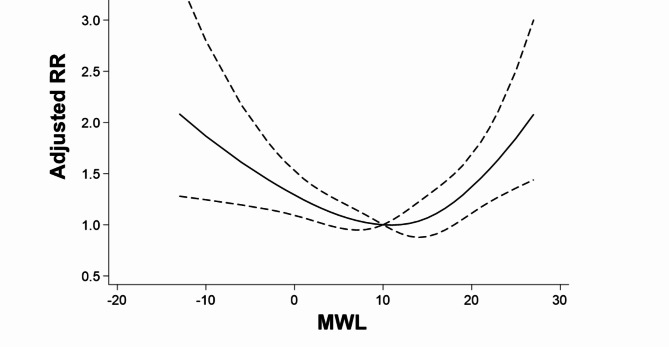
In a single-center, retrospective cohort study at Okayama Medical Center, we evaluated data from extremely preterm infants admitted to the neonatal intensive care unit from 2010 to 2020. Infants who died within the first 10 days of life were excluded. MWL in the first 10 days was the main exposure, categorized into three groups: >15%, 5-15%, and < 5%. The primary outcome evaluated was the occurrence of death or neurodevelopmental impairment (NDI) at age 3 years, defined as developmental impairments (developmental quotient [DQ] < 85), cerebral palsy, hearing impairments, or visual impairments. Data analysis involved robust Poisson regression, adjusted for perinatal confounders, with a restricted cubic spline function to examine the dose-response relationship. We also conducted a sensitivity analysis using a DQ of < 70 to define developmental impairment.
Among 135 infants assessed for neurodevelopmental outcomes, 40 were in the > 15% MWL group, 71 in the 5-15% group, and 24 in the < 5% group. Median gestational ages and birth weights were 25.9 weeks and 821 g for > 15% MWL; 26.1 weeks and 818 g for 5-15% MWL; and 26.0 weeks and 734 g for < 5% MWL. Compared with the 5-15% MWL group, the < 5% group exhibited a higher risk of death or NDI at age 3 years (62.8% vs. 80.8%, risk ratio [RR] 1.36, 95% confidence interval [CI] 1.04-1.79) and NDI alone (59.2% vs. 79.2%, RR 1.43, 95% CI 1.06-1.94). Furthermore, higher risks of developmental impairment were also noted in the > 15% (RR 1.32, 95% CI 1.00-1.75) and < 5% (RR 1.46, 95% CI 1.08-1.98) groups. These associations were confirmed by spline analyses. In contrast, the associations between MWL and neurodevelopmental outcomes using a DQ of < 70 were not apparent.
MWL within the first 10 days of life may be associated with increased risks of NDI and developmental impairments by age 3 years in extremely preterm infants.
先前的研究表明,极低出生体重儿(ELBWI)出生后最大体重损失(MWL)与新生儿死亡率和发病率之间存在相关性。然而,MWL 与神经发育结局之间的关系仍未得到充分探索。
在冈山医疗中心的一项单中心回顾性队列研究中,我们评估了 2010 年至 2020 年入住新生儿重症监护病房的极早产儿的数据。排除出生后 10 天内死亡的婴儿。MWL 在头 10 天内是主要暴露因素,分为三组:>15%、5-15%和<5%。主要结局评估为 3 岁时死亡或神经发育障碍(NDI)的发生,定义为发育障碍(发育商[DQ]<85)、脑瘫、听力障碍或视力障碍。数据分析采用稳健泊松回归,调整围产期混杂因素,采用限制立方样条函数检验剂量-反应关系。我们还使用 DQ<70 来定义发育障碍进行了敏感性分析。
在评估神经发育结局的 135 名婴儿中,40 名在 MWL>15%组,71 名在 5-15%组,24 名在 MWL<5%组。MWL>15%组的中位胎龄和出生体重分别为 25.9 周和 821g;5-15% MWL 组分别为 26.1 周和 818g;MWL<5%组分别为 26.0 周和 734g。与 5-15% MWL 组相比,<5% MWL 组在 3 岁时死亡或 NDI 的风险更高(62.8% vs. 80.8%,风险比[RR]1.36,95%置信区间[CI]1.04-1.79),NDI 发生率更高(59.2% vs. 79.2%,RR 1.43,95% CI 1.06-1.94)。此外,MWL>15%(RR 1.32,95% CI 1.00-1.75)和<5%(RR 1.46,95% CI 1.08-1.98)组也存在更高的发育障碍风险。这些关联通过样条分析得到了证实。相比之下,使用 DQ<70 定义 MWL 与神经发育结局之间的关联并不明显。
极低出生体重儿出生后前 10 天内的 MWL 可能与 3 岁时的 NDI 和发育障碍风险增加有关。