van de Voort Jan C, Vrancken Suzanne M, Manusama Eric R, Borger van der Burg Boudewijn L S, Klinkert Pieter, Hoencamp Rigo
Trauma Research Unit, Department of Trauma Surgery, Erasmus Medical Center, Rotterdam, The Netherlands.
Department of Surgery, Alrijne Hospital Location Leiderdorp, Leiderdorp, The Netherlands.
Trauma Surg Acute Care Open. 2024 Sep 28;9(1):e001515. doi: 10.1136/tsaco-2024-001515. eCollection 2024.
Resuscitative endovascular balloon occlusion of the aorta (REBOA) is increasingly being used for temporary bleeding control in patients with trauma with non-compressible truncal hemorrhage (NCTH). In recent years, the technique is gaining popularity in postpartum hemorrhage and non-traumatic cardiac arrest, although still underutilized. In other surgical fields, however, there is not yet much awareness for the possible advantages of this technique. Consequently, for non-trauma indications, limited data are available.
Description of the use of REBOA in two patients with hemorrhagic shock due to exsanguinating non-traumatic NCTH.
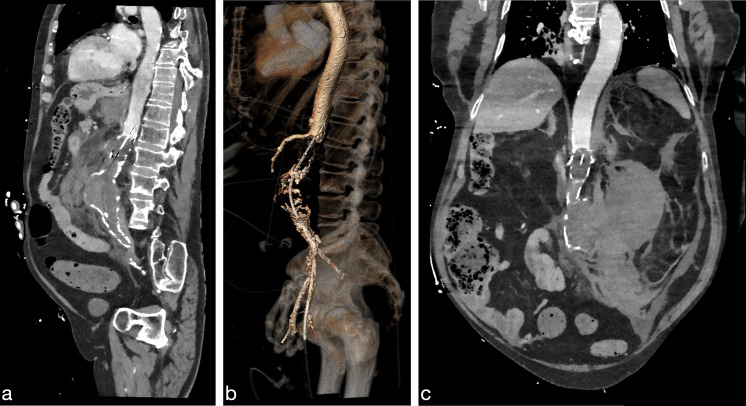
In the first case, REBOA was deployed at the emergency department in a patient in their 80s presenting with hemorrhagic shock due to a ruptured abdominal aortic aneurysm. Hemodynamic stability was obtained and a CT scan was subsequently performed for planning of endovascular aneurysm repair. After successful placement of the endograft, the REBOA catheter was deflated and removed. In the second case, REBOA was performed in a patient with shock due to iatrogenic epigastric artery bleeding after an umbilical hernia repair to prevent hemodynamic collapse and facilitate induction of anesthesia for definitive surgery. During laparotomy, blood pressure-guided intermittent aortic balloon occlusion was used to preserve perfusion of the abdominal organs. Patient made a full recovery.
REBOA deployment was successful in achieving temporary hemorrhage control and hemodynamic stability in patients with non-traumatic NCTH. REBOA facilitated diagnostic work-up, transportation to the operating room and prevented hemodynamic collapse during definitive surgical repair. In the right patient and skilled hands, this relatively simple endovascular procedure could buy precious time and prove lifesaving in a variety of non-compressible hemorrhage.
复苏性血管内主动脉球囊阻断术(REBOA)越来越多地用于控制非压迫性躯干出血(NCTH)创伤患者的临时出血。近年来,该技术在产后出血和非创伤性心脏骤停中越来越受欢迎,尽管仍未得到充分利用。然而,在其他外科领域,对该技术可能的优势认识还不多。因此,对于非创伤性适应症,可用数据有限。
描述REBOA在两名因非创伤性NCTH大出血导致失血性休克患者中的应用。
第一例中,一名80多岁因腹主动脉瘤破裂出现失血性休克的患者在急诊科接受了REBOA治疗。获得了血流动力学稳定,随后进行了CT扫描以规划血管内动脉瘤修复。成功植入血管内支架后,REBOA导管放气并取出。第二例中,一名患者在脐疝修补术后因医源性上腹壁动脉出血出现休克,进行REBOA以防止血流动力学崩溃,并便于为确定性手术诱导麻醉。在剖腹手术期间,使用血压引导的间歇性主动脉球囊阻断来维持腹部器官的灌注。患者完全康复。
REBOA成功地实现了对非创伤性NCTH患者的临时出血控制和血流动力学稳定。REBOA有助于诊断检查、转运至手术室,并在确定性手术修复期间防止血流动力学崩溃。在合适的患者和技术熟练的医生手中,这种相对简单的血管内手术可以赢得宝贵的时间,并在各种不可压迫性出血中挽救生命。