Parke Rachael L, McGuinness Shay P, Cavadino Alana, Cowdrey Keri-Anne, Bates Samantha, Bihari Shailesh, Corley Amanda, Gilder Eileen, Hodgson Carol, Litton Edward, McArthur Colin, Nichol Alistair, Parker Jane, Turner Anne, Webb Steve, Van Haren Frank Mp
Cardiothoracic and Vascular Intensive Care Unit, Te Toka Tumai Auckland, Auckland, New Zealand.
School of Nursing, The University of Auckland, Auckland, New Zealand.
Crit Care Resusc. 2024 Jun 21;26(3):161-168. doi: 10.1016/j.ccrj.2024.05.001. eCollection 2024 Sep.
Acute respiratory distress syndrome (ARDS) is associated with significant mortality, morbidity, and cost. We aimed to describe characteristics and management of adult patients admitted to intensive care units (ICUs) in Australia and New Zealand with moderate-severe ARDS, to better understand contemporary practice.
Bi-national, prospective, observational, multi-centre study.
19 ICUs in Australia and New Zealand.
Mechanically ventilated patients with moderate-severe ARDS.
Baseline demographic characteristics, ventilation characteristics, use of adjunctive support therapy and all-cause mortality to day 28. Data were summarised using descriptive statistics.
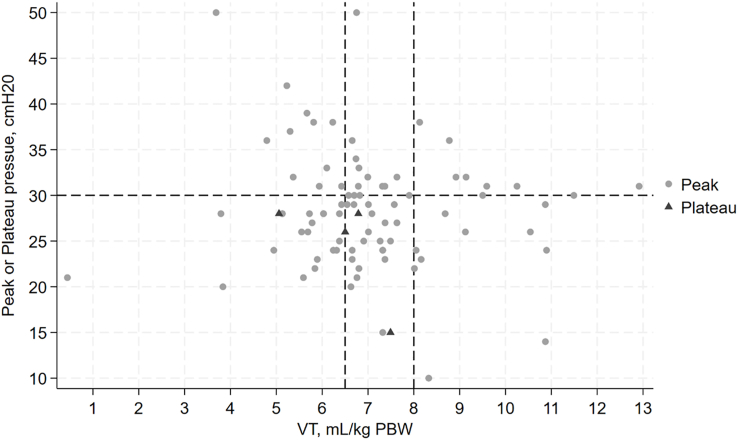
200 participants were enrolled, mean (±SD) age 55.5 (±15.9) years, 40% (n = 80) female. Around half (51.5%) had no baseline comorbidities and 45 (31%) tested positive for COVID-19. On day 1, mean SOFA score was 9 ± 3; median (IQR) PaO/FiO ratio 119 (89, 142), median (IQR) FiO 70% (50%, 99%) and mean (±SD) positive end expiratory pressure (PEEP) 11 (±3) cmHO. On day one, 10.5% (n = 21) received lung protective ventilation (LPV) (tidal volume ≤6.5 mL/kg predicted body weight and plateau pressure or peak pressure ≤30 cm HO). Adjunctive therapies were received by 86% (n = 172) of patients at some stage from enrolment to day 28. Systemic steroids were most used (n = 127) followed by neuromuscular blockers (n = 122) and prone positioning (n = 27). Median ventilator-free days (IQR) to day 28 was 5 (0, 20). In-hospital mortality, censored at day 28, was 30.5% (n = 61).
In Australia and New Zealand, compliance with evidence-based practices including LPV and prone positioning was low in this cohort. Therapies with proven benefit in the treatment of patients with moderate-severe ARDS, such as lung protective ventilation and prone positioning, were not routinely employed.
急性呼吸窘迫综合征(ARDS)与显著的死亡率、发病率和成本相关。我们旨在描述澳大利亚和新西兰重症监护病房(ICU)收治的中重度ARDS成年患者的特征和管理情况,以更好地了解当代的治疗实践。
双国家、前瞻性、观察性、多中心研究。
澳大利亚和新西兰的19个ICU。
接受机械通气的中重度ARDS患者。
基线人口统计学特征、通气特征、辅助支持治疗的使用情况以及至第28天的全因死亡率。数据采用描述性统计进行汇总。
共纳入200名参与者,平均(±标准差)年龄55.5(±15.9)岁,40%(n = 80)为女性。约一半(51.5%)患者无基线合并症,45名(31%)患者新冠病毒检测呈阳性。第1天,平均序贯器官衰竭评估(SOFA)评分为9±3;动脉血氧分压/吸入氧分数(PaO/FiO)比值中位数(四分位间距)为119(89,142),吸入氧分数(FiO)中位数(四分位间距)为70%(50%,99%),平均(±标准差)呼气末正压(PEEP)为11(±3)cmH₂O。第1天,10.5%(n = 21)的患者接受了肺保护性通气(LPV)(潮气量≤6.5 mL/kg预计体重,平台压或峰压≤30 cmH₂O)。从入组到第28天的某个阶段,86%(n = 17₂)的患者接受了辅助治疗。使用最多的辅助治疗是全身用类固醇(n = 127),其次是神经肌肉阻滞剂(n = 122)和俯卧位通气(n = 27)。至第28天无呼吸机天数中位数(四分位间距)为5(0,20)。以第28天为截尾时间,住院死亡率为30.5%(n = 61)。
在澳大利亚和新西兰,该队列中对包括LPV和俯卧位通气在内的循证实践的依从性较低。在治疗中重度ARDS患者时已证实有获益的治疗方法,如肺保护性通气和俯卧位通气,未被常规采用。