Department of Orthopedic Surgery, Yamaguchi University Graduate School of Medicine, Ube, Yamaguchi, 755-8505, Japan.
Department of Orthopedic Surgery, Yamaguchi Prefectural Grand Medical Center, Hofu, Yamaguchi, 747-8511, Japan.
BMC Musculoskelet Disord. 2024 Oct 4;25(1):787. doi: 10.1186/s12891-024-07891-3.
A robotic arm-assisted and a computed tomography (CT)- based navigation system have been reported to improve the accuracy of component positioning in total hip arthroplasty (THA). However, no study has compared robotic arm-assisted THA (rTHA) to CT-based navigated THA (nTHA) concerning accuracy of cup placement and acetabular fractures using the direct anterior approach (DAA). This study aimed to compare the accuracy of cup placement and the presence of intraoperative acetabular fractures between rTHA and nTHA using DAA in the supine position.
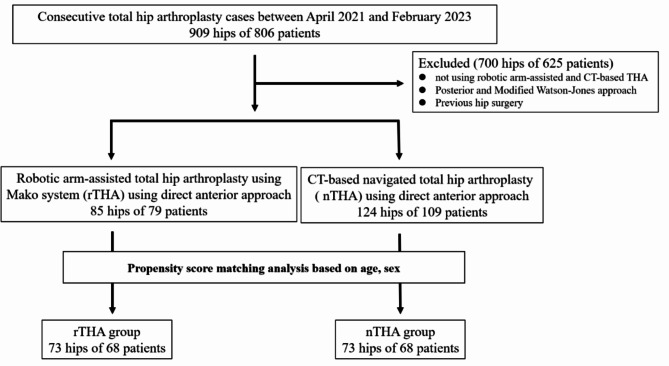
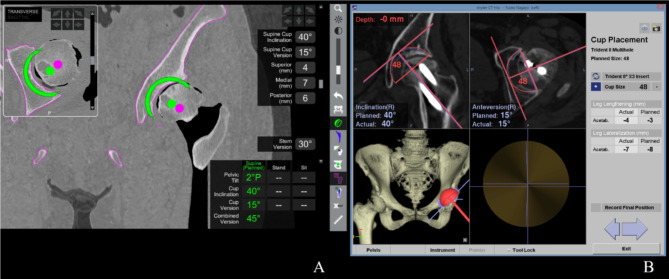
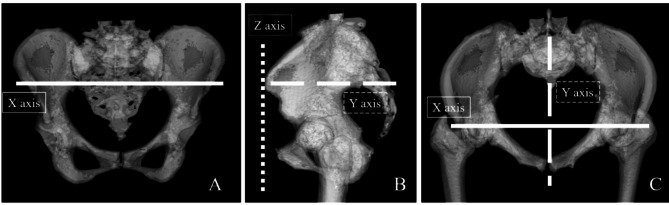
We retrospectively investigated 209 hips of 188 patients who underwent rTHA or nTHA using DAA (rTHA using the Mako system: 85 hips of 79 patients; nTHA: 124 hips of 109 patients). After propensity score matching for age and sex, each group consisted of 73 hips. We evaluated clinical and radiographic outcomes, comparing postoperative cup orientation and position, measured using a three-dimensional templating software, to preoperative CT planning. Additionally, we investigated the prevalence of occult acetabular fracture.
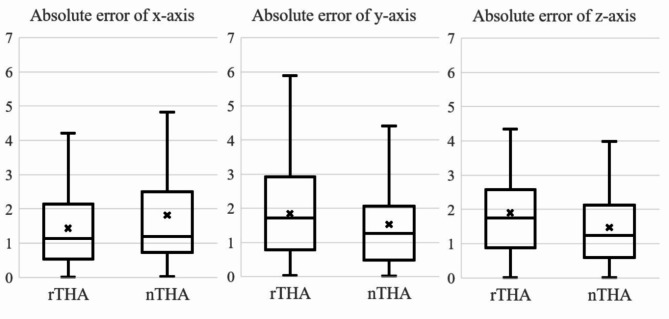
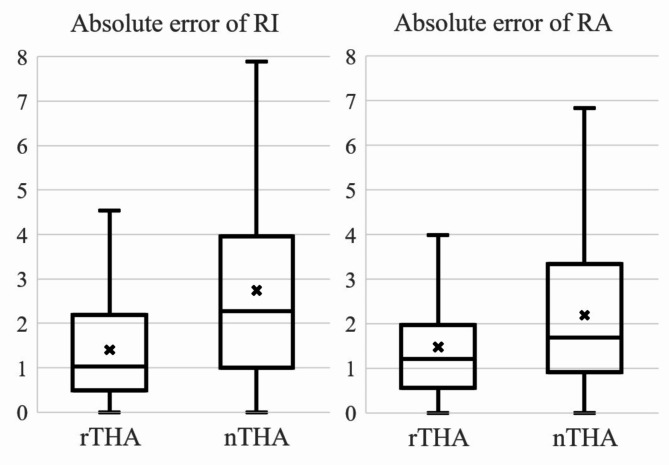
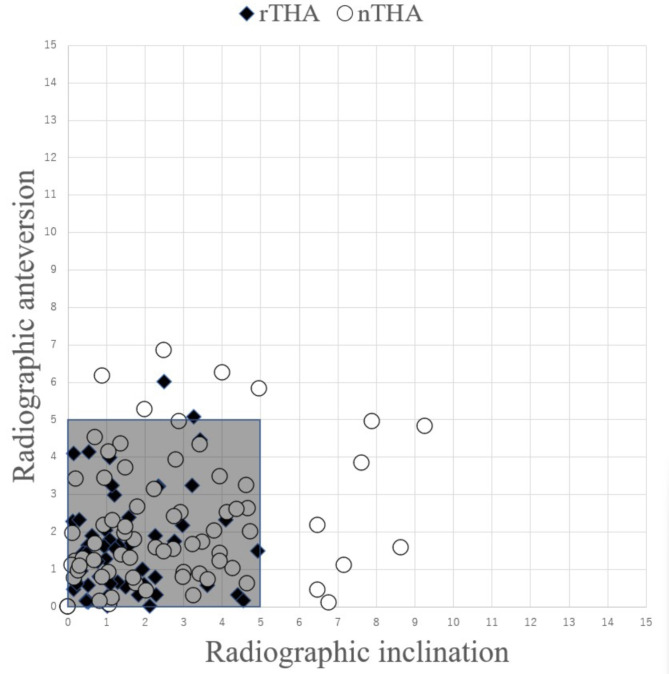
Clinical outcomes were not significantly different between the groups at 1 year postoperatively. The mean absolute error of cup orientation was significantly smaller in the rTHA group than in nTHA (inclination: 1.4° ± 1.2° vs. 2.7° ± 2.2°, respectively; p = 0.0001, anteversion: 1.5° ± 1.3° vs. 2.2° ± 1.7°, respectively; p = 0.007). The cases within an absolute error of 5 degrees in both RI and RA were significantly higher in the rTHA (97.3%) than in nTHA group (82.2%) (p = 0.003). The absolute error of the cup position was not significantly different between the two groups. The prevalence of occult acetabular fracture did not differ significantly between the two groups (rTHA: n = 0 [0%] vs. nTHA: n = 1 [1.4%]).
Cup placement using DAA in the supine position in rTHA was more accurate with fewer outliers compared to nTHA. Therefore, rTHA performed via DAA in a supine position would be useful for accurate cup placement.
机器人辅助和计算机断层扫描(CT)导航系统已被报道可提高全髋关节置换术(THA)中关节组件定位的准确性。然而,尚无研究比较机器人辅助 THA(rTHA)与 CT 导航 THA(nTHA)在仰卧位直接前入路(DAA)中髋臼杯放置的准确性和髋臼骨折的发生率。本研究旨在比较 rTHA 和 nTHA 在 DAA 下仰卧位的髋臼杯放置精度和术中髋臼骨折的发生率。
我们回顾性调查了 188 名患者的 209 髋接受 rTHA 或 nTHA (rTHA 使用 Mako 系统:79 名患者 85 髋;nTHA:109 名患者 124 髋)。在年龄和性别进行倾向评分匹配后,每组各 73 髋。我们评估了临床和影像学结果,使用三维模板软件比较术后髋臼杯的方向和位置,与术前 CT 规划进行比较。此外,我们还研究了隐匿性髋臼骨折的发生率。
术后 1 年,两组的临床结果无显著差异。rTHA 组髋臼杯方向的平均绝对误差明显小于 nTHA 组(倾斜度:分别为 1.4°±1.2°和 2.7°±2.2°;p=0.0001,前倾角:分别为 1.5°±1.3°和 2.2°±1.7°;p=0.007)。rTHA 组 RI 和 RA 内的髋臼杯位置的绝对误差在 5 度以内的病例明显高于 nTHA 组(97.3%比 82.2%)(p=0.003)。两组髋臼杯位置的绝对误差无显著差异。两组隐匿性髋臼骨折的发生率无显著差异(rTHA:n=0 [0%] vs. nTHA:n=1 [1.4%])。
与 nTHA 相比,仰卧位 DAA 下的 rTHA 髋臼杯位置更准确,离群值更少。因此,仰卧位 DAA 下的 rTHA 可用于准确放置髋臼杯。