Gemzell-Danielsson Kristina, Lindh Ingela, Brynhildsen Jan, Christensson Anna, Moberg Klas, Wernersson Emma, Johansson Susanne
Department of Women's and Children's Health, Karolinska Institutet, Stockholm, Sweden
Department of Obstetrics and Gynecology, Sahlgrenska Academy at Gothenburg University, Sahlgrenska University Hospital, Gothenburg, Sweden.
BMJ Sex Reprod Health. 2025 Jul 10;51(3):221-231. doi: 10.1136/bmjsrh-2024-202302.
In many countries, persons seeking medical abortion with mifepristone followed by misoprostol can self-administer the second drug, misoprostol, at home, but self-administration of the first drug, mifepristone, is not allowed to the same extent.
This systematic review aims to evaluate whether the efficacy, safety and women's satisfaction with abortion treatment are affected when mifepristone is self-administered at home instead of in a clinic.
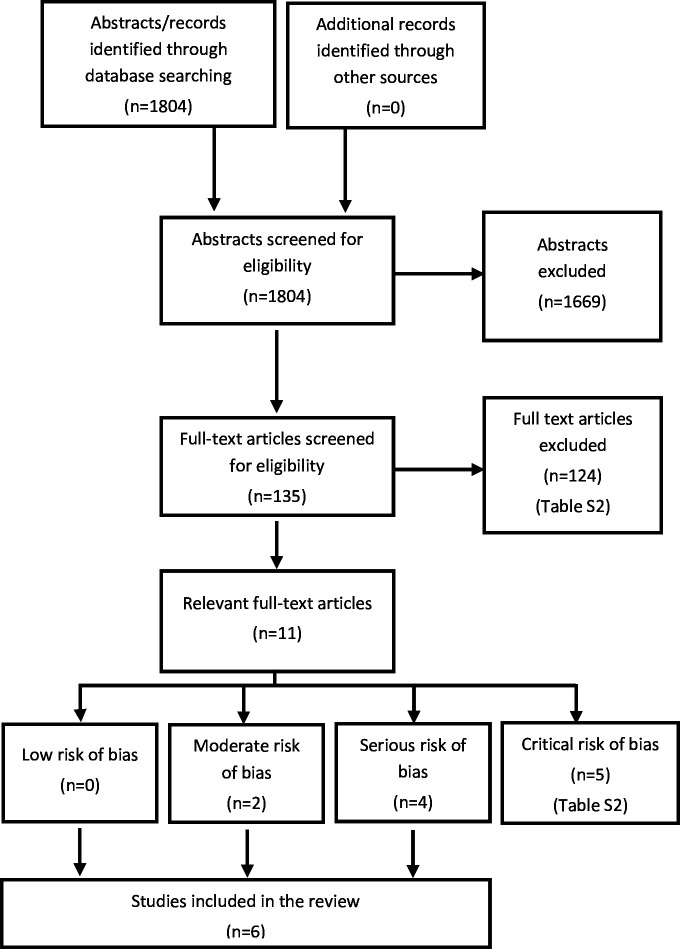
A literature search covered CINAHL, Cochrane Library, Embase, Ovid MEDLINE and APA PsycInfo in October 2022.
Eligible studies focused on persons undergoing medical abortion comparing home and in-clinic mifepristone intake. Outcomes included abortion effectiveness, compliance, acceptability, and practical consequences for women.
Two reviewers independently assessed eligibility and risk of bias. Meta-analysis included similar studies while those differing in design were synthesised without meta-analysis.
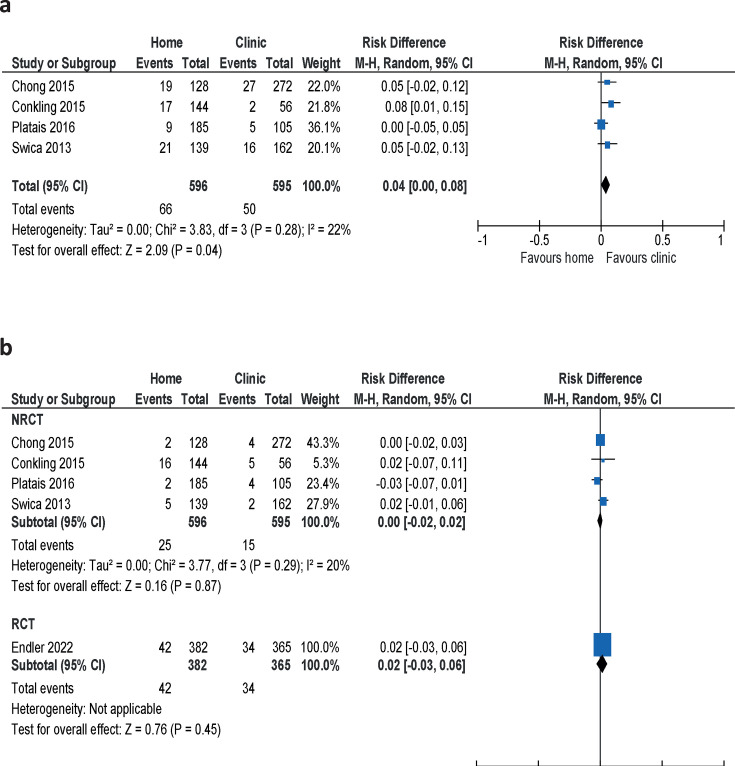
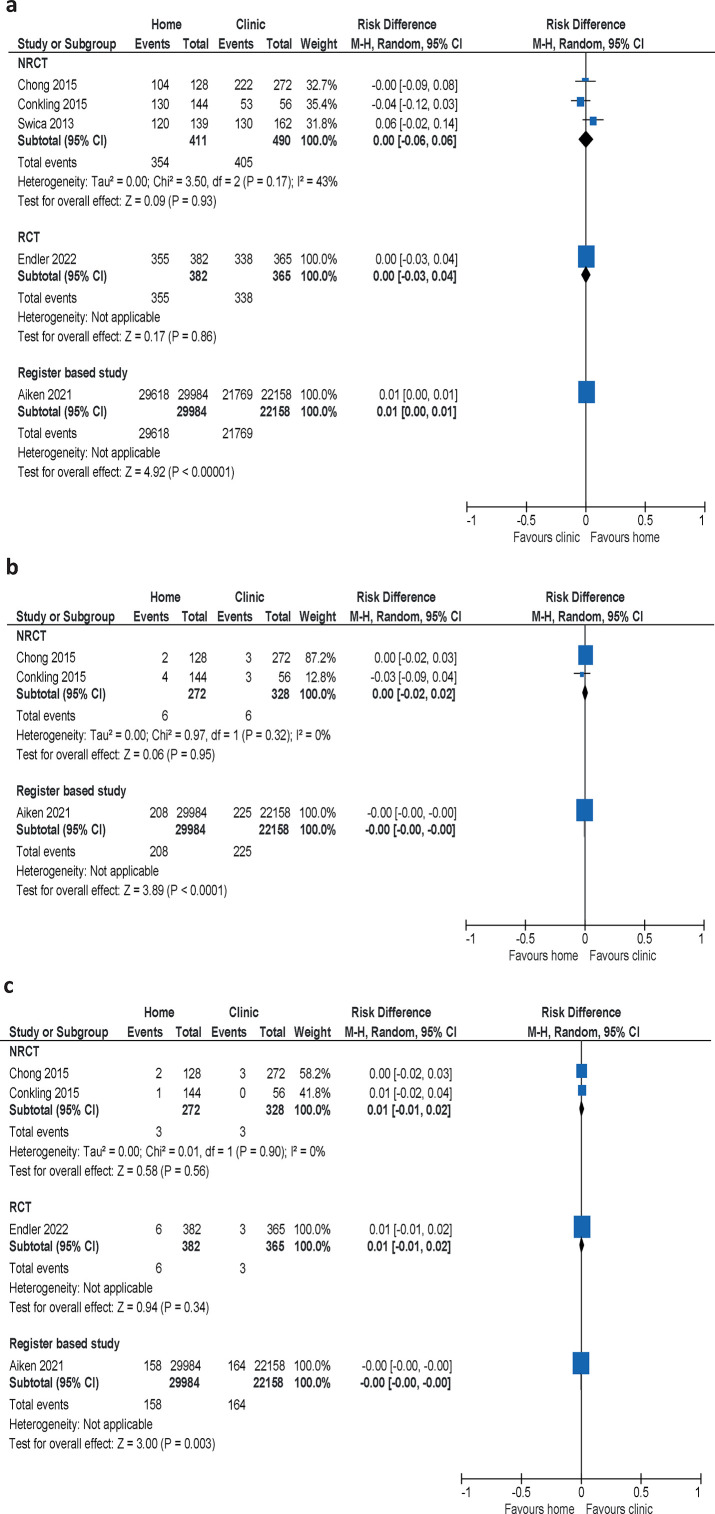
Six studies (54 233 women) of medical abortions up to 10 weeks were included. One randomised controlled trial and one retrospective register study had moderate risk of bias, and four non-randomised clinical trials where women could choose the place for intake of mifepristone had serious risk of bias. There was no difference in abortion effectiveness (high confidence) or compliance (moderate confidence) between mifepristone administered at home or in-clinic. No differences in complications were detected between groups and most women who chose home administration of mifepristone expressed a preference for this approach.
Our systematic review demonstrates that the effectiveness of medical abortion is comparable regardless of mifepristone administration and intake, at home or in the clinic.
在许多国家,寻求米非司酮序贯米索前列醇药物流产的人可以在家自行服用第二种药物米索前列醇,但第一种药物米非司酮的自行服用在同等程度上是不被允许的。
本系统评价旨在评估在家而非在诊所自行服用米非司酮时,药物流产的疗效、安全性及女性对流产治疗的满意度是否会受到影响。
2022年10月对CINAHL、考克兰图书馆、Embase、Ovid MEDLINE和美国心理学会心理学文摘数据库进行了文献检索。
符合条件的研究聚焦于接受药物流产的人,比较在家和在诊所服用米非司酮的情况。结局包括流产效果、依从性、可接受性以及对女性的实际影响。
两名评价员独立评估研究的入选资格和偏倚风险。荟萃分析纳入了相似的研究,而设计不同的研究则在没有荟萃分析的情况下进行综合分析。
纳入了6项关于妊娠10周以内药物流产的研究(共54233名女性)。1项随机对照试验和1项回顾性登记研究存在中度偏倚风险,4项非随机临床试验中女性可选择米非司酮的服用地点,存在严重偏倚风险。在家或在诊所服用米非司酮,流产效果(高可信度)或依从性(中度可信度)没有差异。两组间未检测到并发症差异,大多数选择在家服用米非司酮的女性表示更喜欢这种方式。
我们通过系统评价表明,无论米非司酮是在家还是在诊所服用,药物流产的效果都是相当的。