Boekel Naomi B, Duane Fran K, Jacobse Judy N, Hauptmann Michael, Schaapveld Michael, Sonke Gabe S, Gietema Jourik A, Hooning Maartje J, Seynaeve Caroline M, Maas Angela H E M, Darby Sarah C, Aleman Berthe M P, Taylor Carolyn W, van Leeuwen Flora E
Epidemiology, Netherlands Cancer Institute, Amsterdam, The Netherlands.
Medical Research Council Population Health Research Unit, University of Oxford, Oxford, UK.
Eur J Heart Fail. 2020 Feb;22(2):366-374. doi: 10.1002/ejhf.1620. Epub 2019 Nov 12.
We aimed to develop dose-response relationships for heart failure (HF) following radiation and anthracyclines in breast cancer treatment, and to assess HF associations with trastuzumab and endocrine therapies.
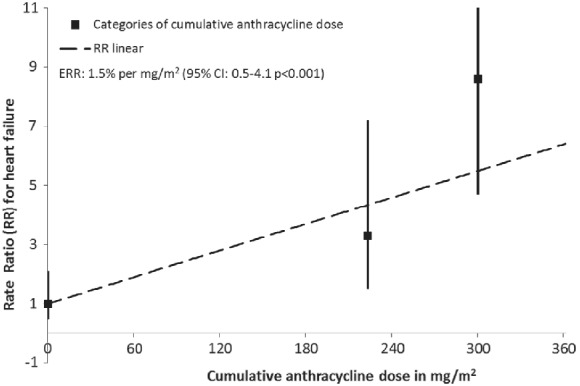
A case-control study was performed within a cohort of breast cancer survivors treated during 1980-2009. Cases (n = 102) had HF as first cardiovascular diagnosis and were matched 1:3 on age and date of diagnosis. Individual cardiac radiation doses were estimated, and anthracycline doses and use of trastuzumab and endocrine therapy were abstracted from oncology notes. For HF cases who received radiotherapy, the estimated median mean heart dose (MHD) was 6.8 Gy [interquartile range (IQR) 0.9-13.7]. MHD was not associated with HF risk overall [excess rate ratio (ERR) = 1%/Gy, 95% confidence interval (CI) -2 to 10]. In patients treated with anthracyclines, exposure of ≥20% of the heart to ≥20 Gy was associated with a rate ratio of 5.7 (95% CI 1.7-21.7) compared to <10% exposed to ≥20 Gy. For cases who received radiotherapy, median cumulative anthracycline dose was 247 mg/m (IQR 240-319). A dose-dependent increase was observed after anthracycline without trastuzumab (ERR = 1.5% per mg/m , 95% CI 0.5-4.1). After anthracycline and trastuzumab, the rate ratio was 34.9 (95% CI 11.1-110.1) compared to no chemotherapy.
In absence of anthracyclines, breast cancer radiotherapy was not associated with increased HF risk. Strongly elevated HF risks were observed after treatment with anthracyclines and also after treatment with trastuzumab. The benefits of these systemic treatments usually exceed the risks of HF, but our results emphasize the need to support ongoing efforts to evaluate preventative strategies.
我们旨在建立乳腺癌治疗中放疗和蒽环类药物治疗后心力衰竭(HF)的剂量-反应关系,并评估HF与曲妥珠单抗和内分泌治疗的关联。
在1980 - 2009年接受治疗的乳腺癌幸存者队列中进行了一项病例对照研究。病例组(n = 102)以HF作为首次心血管诊断,按年龄和诊断日期1:3匹配对照组。估计个体心脏放疗剂量,并从肿瘤学记录中提取蒽环类药物剂量以及曲妥珠单抗和内分泌治疗的使用情况。对于接受放疗的HF病例,估计的中位平均心脏剂量(MHD)为6.8 Gy[四分位间距(IQR)0.9 - 13.7]。总体而言,MHD与HF风险无关[超额率比(ERR)= 1%/Gy,95%置信区间(CI)-2至10]。在接受蒽环类药物治疗的患者中,≥20%的心脏暴露于≥20 Gy与<10%暴露于≥20 Gy相比,率比为5.7(95% CI 1.7 - 21.7)。对于接受放疗的病例,中位累积蒽环类药物剂量为247 mg/m²(IQR 240 - 319)。在未使用曲妥珠单抗的蒽环类药物治疗后观察到剂量依赖性增加(ERR = 每mg/m² 1.5%,95% CI 0.5 - 4.1)。与未进行化疗相比,在蒽环类药物和曲妥珠单抗治疗后,率比为34.9(95% CI 11.1 - 110.1)。
在没有蒽环类药物的情况下,乳腺癌放疗与HF风险增加无关。在蒽环类药物治疗后以及曲妥珠单抗治疗后均观察到HF风险显著升高。这些全身治疗的益处通常超过HF风险,但我们的结果强调需要支持正在进行的评估预防策略的努力。