Ledwaba Leshego, Saidu Rakiya, Malila Bessie, Kuhn Louise, Mutsvangwa Tinashe E M
Division of Biomedical Engineering, Department of Human Biology, Faculty of Health Sciences, University of Cape Town, Cape Town, Western Cape, South Africa.
Obstetrics and Gynaecology, Groote Schuur Hospital/University of Cape Town, Cape Town, Western Cape, South Africa.
medRxiv. 2024 Sep 27:2024.09.27.24314466. doi: 10.1101/2024.09.27.24314466.
Cervical cancer screening programs are poorly implemented in LMICs due to a shortage of specialists and expensive diagnostic infrastructure. To address the barriers of implementation researchers have been developing low-cost portable devices and automating image analysis for decision support.However, as the knowledge base is growing rapidly, progress on the implementation status of novel imaging devices and algorithms in cervical cancer screening has become unclear. The aim of this project was to provide a systematic review summarizing the full range of automated technology systems used in cervical cancer screening.
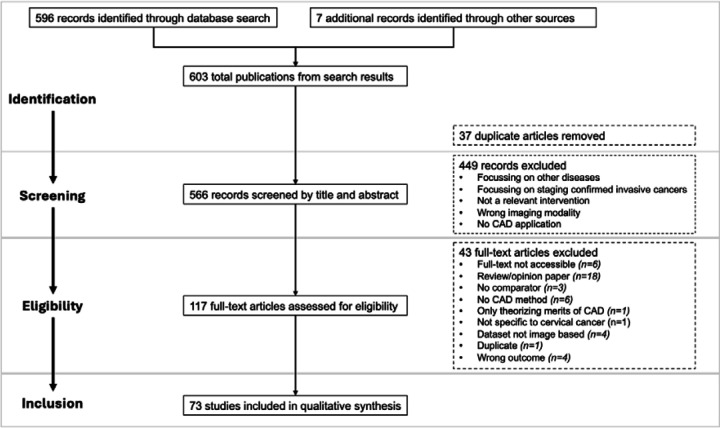
A search on academic databases was conducted and the search results were screened by two independent reviewers. Study selection was based on eligibility in meeting the terms of inclusion and exclusion criteria which were outlined using a Population, Intervention, Comparator and Outcome framework.
17 studies reported algorithms developed with source images from mobile device, viz. Pocket Colposcope, MobileODT EVA Colpo, Smartphone Camera, Smartphone-based Endoscope System, Smartscope, mHRME, and PiHRME. While 56 studies reported algorithms with source images from conventional/commercial acquisition devices. Most interventions were in the feasibility stage of development, undergoing initial clinical validations.
Researchers have proven superior prediction performance of computer aided diagnostics (CAD) in colposcopy (>80% accuracies) versus manual analysis (<70.0% accuracies). Furthermore, this review summarized evidence of the algorithms which are being created utilizing portable devices, to circumvent constraints prohibiting wider implementation in LMICs (such as expensive diagnostic infrastructure). However clinical validation of novel devices with CAD is not yet implemented adequately in LMICs.
由于缺乏专业人员以及诊断基础设施成本高昂,低收入和中等收入国家的宫颈癌筛查项目实施情况不佳。为解决实施障碍,研究人员一直在开发低成本便携式设备并实现图像分析自动化以提供决策支持。然而,随着知识库的迅速增长,新型成像设备和算法在宫颈癌筛查中的实施进展变得不明确。本项目的目的是提供一项系统综述,总结宫颈癌筛查中使用的全系列自动化技术系统。
对学术数据库进行了检索,检索结果由两名独立评审员进行筛选。研究选择基于是否符合使用人群、干预措施、对照和结局框架概述的纳入和排除标准。
17项研究报告了利用移动设备源图像开发的算法,即袖珍阴道镜、MobileODT EVA阴道镜、智能手机摄像头、基于智能手机的内窥镜系统、智能显微镜、多光子反射显微镜扩展成像(mHRME)和偏振多光子反射显微镜扩展成像(PiHRME)。而56项研究报告了使用传统/商业采集设备源图像开发的算法。大多数干预措施处于开发的可行性阶段,正在进行初步临床验证。
研究人员已证明计算机辅助诊断(CAD)在阴道镜检查中的预测性能优于手动分析(准确率>80%对<70.0%)。此外,本综述总结了利用便携式设备创建算法的证据,以规避阻碍在低收入和中等收入国家更广泛实施的限制(如昂贵的诊断基础设施)。然而,低收入和中等收入国家尚未充分对新型CAD设备进行临床验证。