Jin Kecheng, Mi Ningning, He Wangping, Zhong Ruyang, Jin Boru, Liu Zhen, Dong Chunlu, Lin Yanyan, Yue Ping, Xia Bin, He Qiangsheng, Yuan Jinqiu, Meng Wenbo
The First School of Clinical Medicine, Lanzhou University, Lanzhou, China.
Department of General Surgery, The First Hospital of Lanzhou University, Lanzhou, China.
Front Nutr. 2024 Sep 27;11:1469789. doi: 10.3389/fnut.2024.1469789. eCollection 2024.
Limited epidemiological evidence exists concerning the impact of healthy dietary patterns on reducing the risk of cholelithiasis. We aimed to examine the association of seven established dietary patterns with subsequent cholelithiasis risk and whether this association was modified by genetic risk.
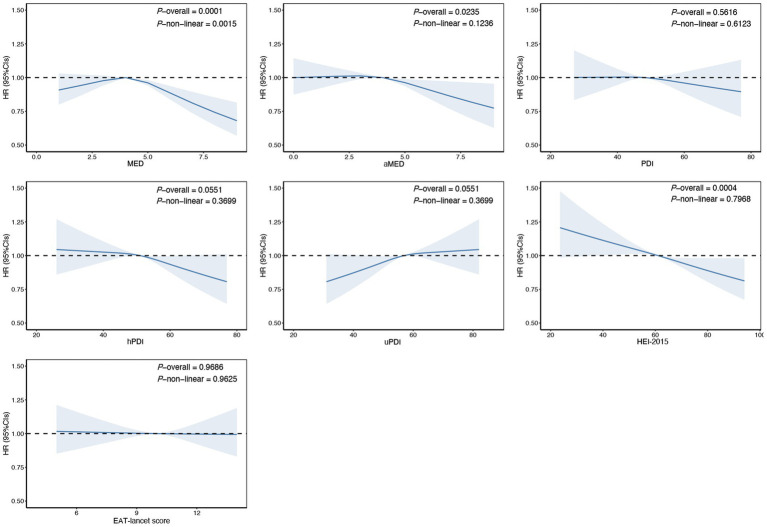
We conducted a prospective cohort study from the UK Biobank, including 155,323 participants initially free of cholelithiasis and cholecystectomy. Dietary patterns were assessed using a validated food frequency questionnaire (Oxford WebQ), covering Mediterranean Diet Score (MED), alternate Mediterranean Diet Score(aMED), overall Plant-based Diet Index (PDI), healthy Plant-based Diet Index (hPDI), unhealthy Plant-based Diet Index (uPDI), Healthy Eating Index 2015 (HEI-2015) and EAT-lancet Score. Genetic risk was quantified and stratified by a polygenic risk score (PRS) incorporating 13 known cholelithiasis-associated loci. Cox proportional hazards regression was employed to estimate the association between dietary patterns, PRS, and cholelithiasis incidence, adjusting for potential confounders.
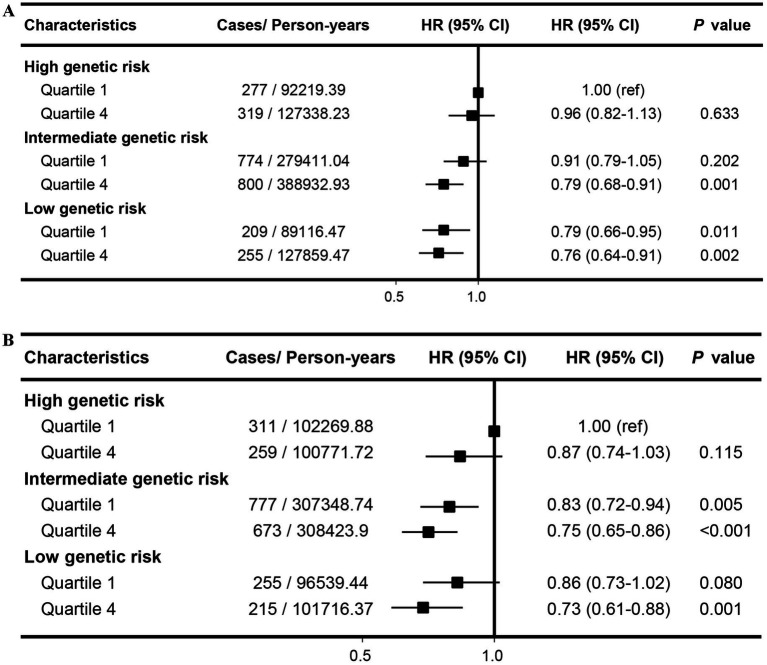
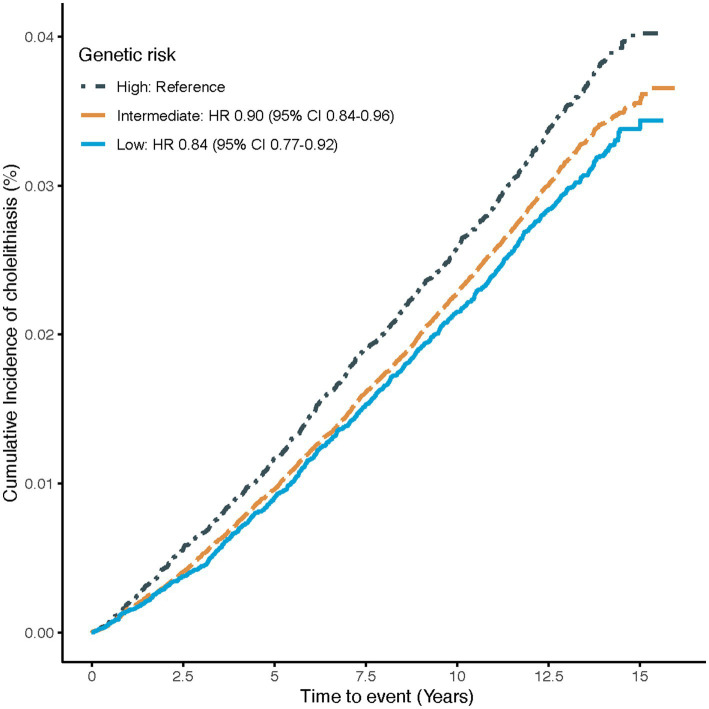
During a median follow-up of 13.3 years, 5,056 cases of cholelithiasis were identified. After adjusting for potential confounders, adherence to aMED and HEI-2015 dietary patterns reduced cholelithiasis risk by 10% (HR: 0.90; 95%CI: 0.83-0.98) and 11% (HR: 0.89; 95%CI: 0.82-0.96), respectively. A significant decrease in cholelithiasis risk was observed across PRS quintiles, low PRS was associated with a 16% reduced risk (HR: 0.84; 95%CI: 0.77-0.92). Participants with both high dietary scores and low genetic risk had the lowest cholelithiasis risk, with an HR of 0.76 (95%CI: 0.64-0.91) for aMED and 0.73 (95%CI: 0.61-0.88) for HEI-2015.
Higher adherence to aMED and HEI-2015 might significantly decrease the risk of cholelithiasis, irrespective of genetic risk. Our results highlighted the potential of diet intervention for cholelithiasis prevention in the general population.
关于健康饮食模式对降低胆结石风险的影响,流行病学证据有限。我们旨在研究七种既定饮食模式与后续胆结石风险之间的关联,以及这种关联是否会因遗传风险而改变。
我们对英国生物银行进行了一项前瞻性队列研究,纳入了155323名最初无胆结石和胆囊切除术的参与者。使用经过验证的食物频率问卷(牛津网络问卷)评估饮食模式,涵盖地中海饮食评分(MED)、替代地中海饮食评分(aMED)、总体植物性饮食指数(PDI)、健康植物性饮食指数(hPDI)、不健康植物性饮食指数(uPDI)、2015年健康饮食指数(HEI - 2015)和EAT - 柳叶刀评分。通过纳入13个已知胆结石相关位点的多基因风险评分(PRS)对遗传风险进行量化和分层。采用Cox比例风险回归来估计饮食模式、PRS与胆结石发病率之间的关联,并对潜在混杂因素进行调整。
在中位随访13.3年期间,共确定了5056例胆结石病例。在调整潜在混杂因素后,坚持aMED和HEI - 2015饮食模式分别使胆结石风险降低了10%(HR:0.90;95%CI:0.83 - 0.98)和11%(HR:0.89;95%CI:0.82 - 0.96)。在PRS五分位数中观察到胆结石风险显著降低,低PRS与风险降低16%相关(HR:0.84;95%CI:0.77 - 0.92)。饮食评分高且遗传风险低的参与者胆结石风险最低,aMED的HR为0.76(95%CI:0.64 - 0.91),HEI - 2015的HR为0.73(95%CI:0.61 - 0.88)。
更高程度地坚持aMED和HEI - 2015可能会显著降低胆结石风险,无论遗传风险如何。我们的结果突出了饮食干预在普通人群中预防胆结石的潜力。