Di Michele Stefano, Bramante Silvia, Rosati Maurizio
Division of Gynecology and Obstetrics, Department of Surgical Sciences, University of Cagliari, 09124 Cagliari, Italy.
Unit of Obstetrics and Gynecology, Santo Spirito Hospital, 65124 Pescara, Italy.
J Clin Med. 2024 Sep 24;13(19):5677. doi: 10.3390/jcm13195677.
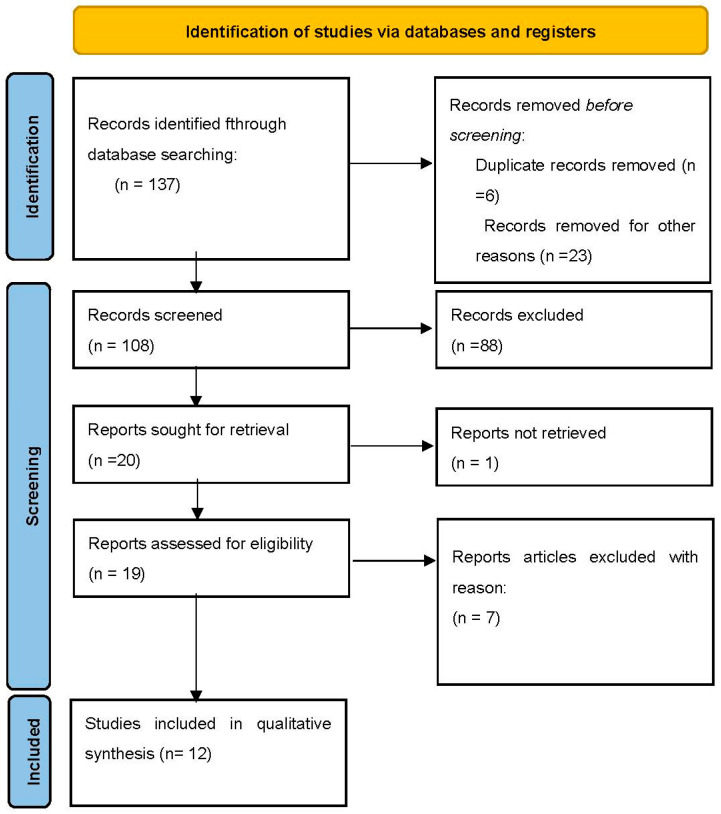
Endometriosis, characterized by the presence of endometrial tissue outside the uterus, includes deep endometriosis (DE), which can affect the urinary tract. Ureteral endometriosis (UE) is a rare but significant manifestation that can lead to ureteral obstruction, hydronephrosis, and potential kidney loss. This systematic review evaluates the effectiveness and outcomes of laparoscopic versus robotic-assisted ureteral reimplantation techniques in patients with UE. A systematic literature search was conducted following PRISMA guidelines across PubMed, MEDLINE, Embase, Web of Science, and the Cochrane Library, from inception to July 2024. Studies included patients with UE who underwent ureteral reimplantation using laparoscopic or robotic-assisted techniques. Data on patient demographics, surgical technique, duration of surgery, complications, follow-up duration, and clinical outcomes were extracted and analyzed. Twelve studies met the inclusion criteria, comprising 225 patients in the laparoscopic group and 24 in the robotic-assisted group. Lich-Gregoir ureteral reimplantation, with or without a psoas hitch, was the predominant technique used. The average surgery duration was 271.1 min for the laparoscopic group and 310.4 min for the robotic-assisted group. Recurrence rates for UE were 2.95% for laparoscopic and 5.9% for robotic-assisted procedures. The robotic-assisted group had a significantly shorter hospital stay (6.7 days vs. 9.1 days, < 0.01). Postoperative complication rates were comparable between the two techniques ( = 0.422). Both laparoscopic and robotic-assisted techniques for ureteral reimplantation in UE are safe and effective, with the choice of technique guided by surgeon expertise and specific clinical scenarios. However, the limited number of robotic cases introduces a bias, despite statistical significance.
子宫内膜异位症的特征是子宫外存在子宫内膜组织,包括深部子宫内膜异位症(DE),其可影响泌尿系统。输尿管子宫内膜异位症(UE)是一种罕见但严重的表现形式,可导致输尿管梗阻、肾积水,并可能导致肾脏丧失。本系统评价评估了腹腔镜与机器人辅助输尿管再植技术在UE患者中的有效性和结局。按照PRISMA指南,从创刊至2024年7月,在PubMed、MEDLINE、Embase、Web of Science和Cochrane图书馆进行了系统的文献检索。纳入的研究包括接受腹腔镜或机器人辅助技术进行输尿管再植的UE患者。提取并分析了患者人口统计学、手术技术、手术时间、并发症、随访时间和临床结局的数据。12项研究符合纳入标准,腹腔镜组有225例患者,机器人辅助组有24例患者。采用的主要技术是Lich-Gregoir输尿管再植术,有无腰大肌固定。腹腔镜组的平均手术时间为271.1分钟,机器人辅助组为310.4分钟。UE的复发率在腹腔镜手术中为2.95%,在机器人辅助手术中为5.9%。机器人辅助组的住院时间明显更短(6.7天对9.1天,<0.01)。两种技术的术后并发症发生率相当(=0.422)。UE的腹腔镜和机器人辅助输尿管再植技术均安全有效,技术选择由外科医生的专业知识和具体临床情况指导。然而,尽管具有统计学意义,但机器人手术病例数量有限存在偏倚。