Huntsman Cancer Institute, University of Utah, Salt Lake City, UT, USA.
Fred Hutchinson Cancer Center, Seattle, WA, USA.
Blood Cancer J. 2024 Oct 16;14(1):180. doi: 10.1038/s41408-024-01167-8.
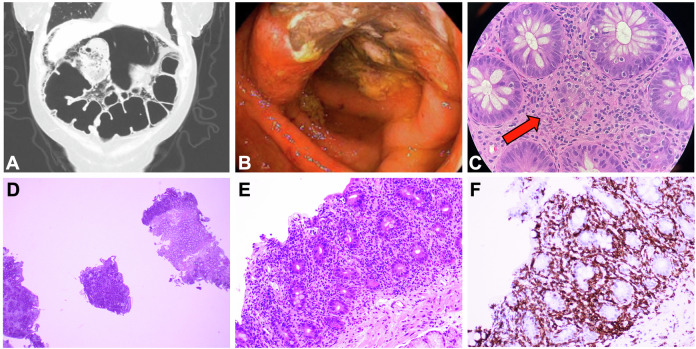
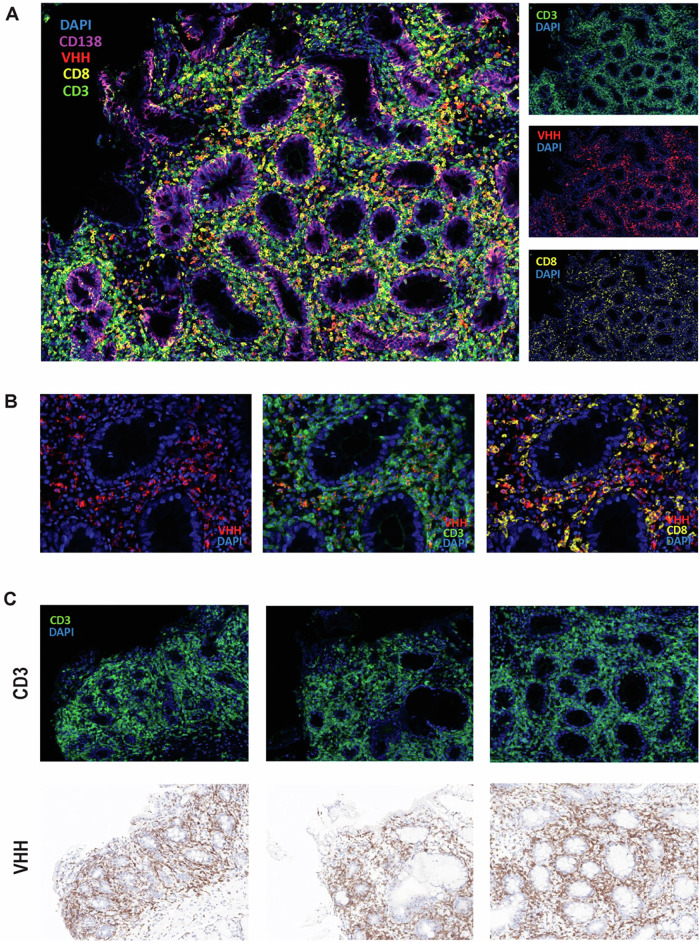
We report 14 cases of immune effector cell (IEC)-associated enterocolitis following chimeric antigen receptor T-cell (CAR-T) therapy in multiple myeloma, with a 1.2% incidence overall (0.2% for idecabtagene vicleucel and 2.2% for ciltacabtagene autoleucel). Patients developed acute-onset symptoms (typically non-bloody Grade 3+ diarrhea) with negative infectious workup beginning a median of 92.5 days (range: 22-210 days) after CAR-T therapy and a median of 85 days after cytokine release syndrome resolution. Gut biopsies uniformly demonstrated inflammation, including intra-epithelial lymphocytosis and villous blunting. In one case where CAR-specific immunofluorescence stains were available, CAR T-cell presence was confirmed within the lamina propria. Systemic corticosteroids were initiated in 10 patients (71%) a median of 25.5 days following symptom onset, with symptom improvement in 40%. Subsequent infliximab or vedolizumab led to improvement in 50% and 33% of corticosteroid-refractory patients, respectively. Five patients (36%) have died from bowel perforation or treatment-emergent sepsis. In conclusion, IEC-associated enterocolitis is a distinct but rare complication of CAR-T therapy typically beginning 1-3 months after infusion. Thorough diagnostic workup is essential, including evaluation for potential T-cell malignancies. The early use of infliximab or vedolizumab may potentially hasten symptom resolution and lower reliance on high-dose corticosteroids during the post-CAR-T period.
我们报告了 14 例多发性骨髓瘤嵌合抗原受体 T 细胞(CAR-T)治疗后免疫效应细胞(IEC)相关性肠炎病例,总发生率为 1.2%(idecabtagene vicleucel 为 0.2%,cilta-cabtagene autoleucel 为 2.2%)。患者出现急性发作症状(通常为无血便的 3+级腹泻),在 CAR-T 治疗后中位 92.5 天(范围:22-210 天)开始进行阴性感染性检查,在细胞因子释放综合征缓解后中位 85 天出现症状。肠道活检均表现为炎症,包括上皮内淋巴细胞增多和绒毛变钝。在一个可进行 CAR 特异性免疫荧光染色的病例中,在固有层内确认了 CAR T 细胞的存在。在症状出现后中位 25.5 天,10 例患者(71%)开始使用全身性皮质类固醇,其中 40%的患者症状改善。随后使用英夫利昔单抗或维多珠单抗,分别使 50%和 33%的皮质类固醇难治性患者症状改善。5 例患者(36%)因肠穿孔或治疗后脓毒症死亡。总之,IEC 相关性肠炎是 CAR-T 治疗的一种独特但罕见的并发症,通常在输注后 1-3 个月开始。彻底的诊断性检查至关重要,包括对潜在 T 细胞恶性肿瘤的评估。早期使用英夫利昔单抗或维多珠单抗可能会加速症状缓解,并降低 CAR-T 后期间对高剂量皮质类固醇的依赖。