Decker Kevin P, Sanjana Faria, Rizzi Nick, Kramer Mary K, Cerjanic Alexander M, Johnson Curtis L, Martens Christopher R
Department of Kinesiology and Applied Physiology, University of Delaware, Newark, DE, United States.
Department of Biomedical Engineering, University of Delaware, Newark, DE, United States.
Front Physiol. 2024 Oct 2;15:1437973. doi: 10.3389/fphys.2024.1437973. eCollection 2024.
To assess the reliability and validity of measuring resting cerebral blood flow (CBF) and hippocampal CBF using a single-post-labeling delay (PLD) and a multi-PLD pseudo-continuous arterial spin labeling (pCASL) protocol for cerebrovascular reactivity (CVR) testing.
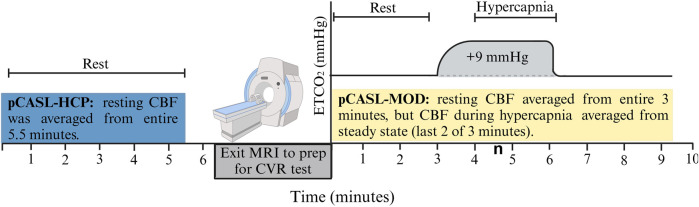
25 healthy, midlife adults (57 ± 4 years old) were imaged in a Siemens Prisma 3T magnetic resonance imaging (MRI) scanner. Resting CBF and hippocampal CBF were assessed using two pCASL protocols, our modified single-PLD protocol (pCASL-MOD) to accommodate the needs for CVR testing and the multi-PLD Human Connectome Project (HCP) Lifespan protocol to serve as the reference control (pCASL-HCP). During pCASL-MOD, CVR was calculated as the change in CBF from rest to hypercapnia (+9 mmHg increase in end-tidal partial pressure of carbon dioxide [PCO]) and then normalized for PCO. The reliability and validity in resting gray matter (GM) CBF, white matter (WM) CBF, and hippocampal CBF between pCASL-MOD and pCASL-HCP protocols were examined using correlation analyses, paired t-tests, and Bland Altman plots.
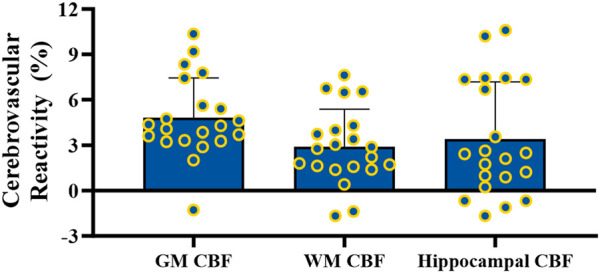
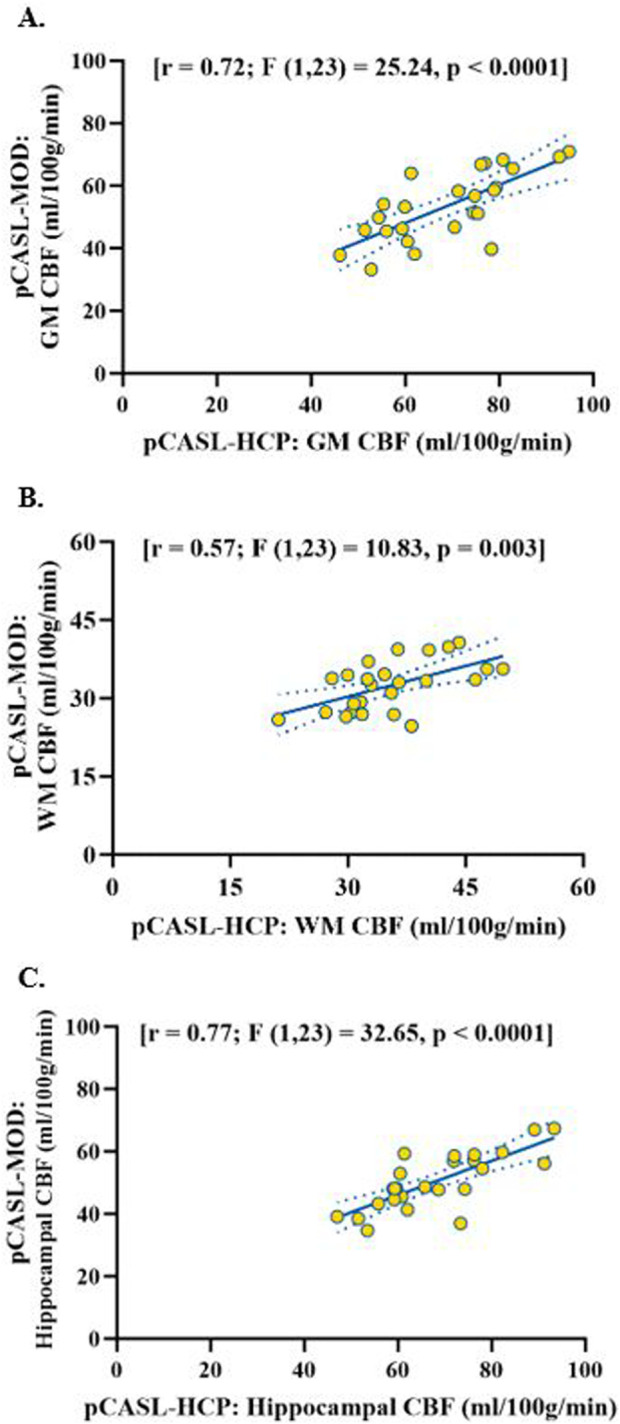
The pCASL-MOD and pCASL-HCP protocols were significantly correlated for resting GM CBF [r = 0.72; F (1, 23) = 25.24, < 0.0001], WM CBF [r = 0.57; F (1, 23) = 10.83, = 0.003], and hippocampal CBF [r = 0.77; F (1, 23) = 32.65, < 0.0001]. However, pCASL-MOD underestimated resting GM CBF (pCASL-MOD: 53.7 ± 11.1 v. pCASL-HCP: 69.1 ± 13.1 mL/100 g/min; < 0.0001), WM CBF (pCASL-MOD: 32.4 ± 4.8 v. pCASL-HCP: 35.5 ± 6.9 mL/100 g/min; = 0.01), and hippocampal CBF (pCASL-MOD: 50.5 ± 9.0 v. pCASL-HCP: 68.1 ± 12.5 mL/100 gmin; < 0.0001). PCO increased by 8.0 ± 0.7 mmHg to induce CVR (GM CBF: 4.8% ± 2.6%; WM CBF 2.9% ± 2.5%; and hippocampal CBF: 3.4% ± 3.8%).
Our single-PLD pCASL-MOD protocol reliably measured CBF and hippocampal CBF at rest given the significant correlation with the multi-PLD pCASL-HCP protocol. Despite the lower magnitude relative to pCASL-HCP, we recommend using our pCASL-MOD protocol for CVR testing in which an exact estimate of CBF is not required such as the assessment of relative change in CBF to hypercapnia.
使用单标记延迟(PLD)和多PLD伪连续动脉自旋标记(pCASL)方案评估静息脑血流量(CBF)和海马CBF测量在脑血管反应性(CVR)测试中的可靠性和有效性。
25名健康的中年成年人(57±4岁)在西门子Prisma 3T磁共振成像(MRI)扫描仪中进行成像。使用两种pCASL方案评估静息CBF和海马CBF,我们改良的单PLD方案(pCASL-MOD)以满足CVR测试的需求,以及多PLD人类连接组计划(HCP)寿命方案作为参考对照(pCASL-HCP)。在pCASL-MOD期间,CVR计算为从静息到高碳酸血症时CBF的变化(呼气末二氧化碳分压[PCO₂]增加9 mmHg),然后针对PCO₂进行标准化。使用相关分析、配对t检验和Bland Altman图检查pCASL-MOD和pCASL-HCP方案之间静息灰质(GM)CBF、白质(WM)CBF和海马CBF的可靠性和有效性。
pCASL-MOD和pCASL-HCP方案在静息GM CBF [r = 0.72;F(1, 23)= 25.24,P < 0.0001]、WM CBF [r = 0.57;F(1, 23)= 10.83,P = 0.003]和海马CBF [r = 0.77;F(1, 23)= 32.65,P < 0.0001]方面显著相关。然而,pCASL-MOD低估了静息GM CBF(pCASL-MOD:53.7±11.1 vs. pCASL-HCP:69.1±13.1 mL/100 g/min;P < 0.000(此处疑似重复,应为P < 0.0001))、WM CBF(pCASL-MOD:32.4±4.8 vs. pCASL-HCP:35.5±6.9 mL/100 g/min;P = 0.01)和海马CBF(pCASL-MOD:50.5±9.0 vs. pCASL-HCP:68.1±12,5 mL/100 gmin;P < 0.0001)。PCO₂增加8.0±0.7 mmHg以诱导CVR(GM CBF:4.8%±2.6%;WM CBF 2.9%±2.5%;海马CBF:3.4%±3.8%)。
鉴于与多PLD pCASL-HCP方案显著相关,我们的单PLD pCASL-MOD方案在静息状态下可靠地测量了CBF和海马CBF。尽管相对于pCASL-HCP幅度较低,但我们建议在不需要精确估计CBF的CVR测试中使用我们的pCASL-MOD方案,例如评估CBF对高碳酸血症的相对变化。