Ghobadi Ali, Hanna Michael, Tovar Stephanie, Do Duy H, Duan Lewei, Lee Ming-Sum, Samuels Elizabeth A, Davis Corey S, Sharp Adam L
Department of Clinical Science Kaiser Permanente Bernard J. Tyson School of Medicine Anaheim California USA.
Kaiser Permanente Southern California Anaheim Medical Center Anaheim California USA.
J Am Coll Emerg Physicians Open. 2024 Oct 17;5(5):e13236. doi: 10.1002/emp2.13236. eCollection 2024 Oct.
Opioid overdose is a public health epidemic adversely impacting individuals and communities. To combat this, California passed a law mandating that prescribers offer a naloxone prescription in certain circumstances. Our objective was to evaluate associations with California's naloxone prescription mandate and emergency department (ED) overdose visits/hospitalizations, opioid and naloxone prescribing, and 30-day mortality.
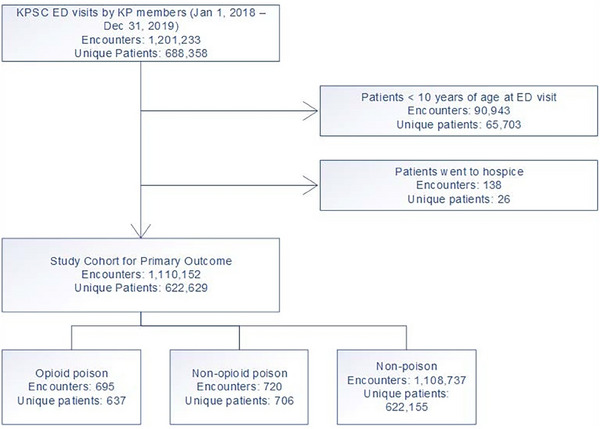
This retrospective cohort study included data from January 1, 2018, to December 31, 2019, and included all Kaiser Permanente Southern California (KPSC) members aged >10 years across 15 KPSC EDs. Exposure was defined as presentation to the ED within the study period. The primary outcome was ED visits for opioid overdose pre- and post-implementation of California's naloxone prescription mandate.
A total of 1.1 million ED visits (534K pre/576K post) were included in the study population. ED opioid overdose visits were 344 (6.4/10,000) pre-policy and 351 (6.1/10,000) post-policy implementation, while non-opioid overdose visits were 309 (5.8/10,000) pre-implementation and 411 (7.1/10,000) post-implementation. The unadjusted rate of visits with opioid prescriptions decreased significantly (14.9% pre to 13.5% post) after implementation. ED naloxone prescriptions increased substantially (104 pre vs. 6031 post). Primary adjusted interrupted time series analysis found no statistical difference between monthly opioid overdose visits pre versus post (odds ratio 1.02, 95% confidence interval [CI] 0.98‒1.07). Difference-in-differences analysis revealed no significant changes in hospitalization (coefficient [CE] = ‒0.05, 95% CI = ‒0.11 to 0.02) or 30-day mortality (CE = ‒0.01, 95% CI = ‒0.03 to 0.01).
This study revealed that the implementation of California's naloxone prescription mandate was associated with significantly increased naloxone prescribing and decreased opioid prescribing, but no significant change in ED opioid overdose visits, hospitalizations, or 30-day mortality. This indicates that increasing naloxone prescribing alone may not be sufficient to lower opioid overdose rates.
阿片类药物过量是一种影响个人和社区的公共卫生流行病。为应对这一问题,加利福尼亚州通过了一项法律,规定在某些情况下,开处方者必须提供纳洛酮处方。我们的目的是评估加利福尼亚州纳洛酮处方规定与急诊科(ED)过量就诊/住院、阿片类药物和纳洛酮处方以及30天死亡率之间的关联。
这项回顾性队列研究纳入了2018年1月1日至2019年12月31日的数据,包括南加利福尼亚州凯撒医疗集团(KPSC)15个急诊科中所有年龄大于10岁的成员。暴露定义为在研究期间到急诊科就诊。主要结局是加利福尼亚州纳洛酮处方规定实施前后因阿片类药物过量到急诊科就诊的情况。
研究人群中共有110万次急诊科就诊(实施前53.4万次/实施后57.6万次)。政策实施前,急诊科阿片类药物过量就诊次数为344次(6.4/10000),实施后为351次(6.1/10000);非阿片类药物过量就诊次数实施前为309次(5.8/10000),实施后为411次(7.1/10000)。实施后,开具阿片类药物处方的就诊率未经调整显著下降(从实施前的14.9%降至实施后的13.5%)。急诊科纳洛酮处方大幅增加(实施前104例,实施后6031例)。初步调整后的中断时间序列分析发现,实施前后每月阿片类药物过量就诊次数无统计学差异(优势比1.02,95%置信区间[CI]0.98‒1.07)。差异分析显示,住院率(系数[CE]=‒0.05,95%CI=‒0.11至0.02)或30天死亡率(CE=‒0.01,95%CI=‒0.03至0.01)无显著变化。
本研究表明,加利福尼亚州纳洛酮处方规定的实施与纳洛酮处方显著增加和阿片类药物处方减少相关,但急诊科阿片类药物过量就诊次数、住院率或30天死亡率无显著变化。这表明仅增加纳洛酮处方可能不足以降低阿片类药物过量率。