Owens Lukas, Brahme Ojas, Gulati Roman, Etzioni Ruth
Division of Public Health Sciences, Fred Hutchinson Cancer Center, Seattle, WA, USA.
JNCI Cancer Spectr. 2024 Nov 1;8(6). doi: 10.1093/jncics/pkae106.
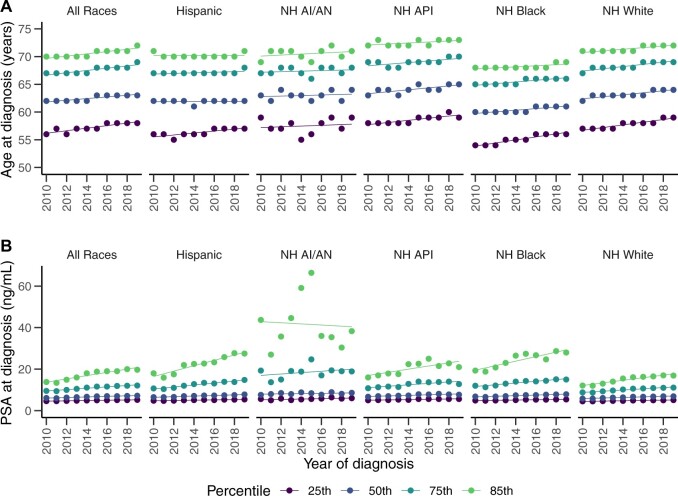
Recent studies have shown that de novo metastatic prostate cancer incidence in the United States increased from 2010 to 2019. Plausible explanations include delayed detection after recommendations against prostate cancer screening or upstaging associated with use of more sensitive imaging technologies. Using Surveillance, Epidemiology, and End Results patient cases and controlling for aging of the population, we found the median age and prostate-specific antigen (PSA) level at prostate cancer diagnosis increased by 1.4 years of age (95% CI = 1.3 to 1.5 years) and 1.4 ng/mL (95% CI = 1.4 to 1.5 ng/mL) over this period, consistent with the delayed detection hypothesis. Racial differences were noted, with 75th percentiles of PSA at diagnosis increasing by 4.3 ng/mL (95% CI = 3.7 to 4.8 ng/mL) over this time period for non-Hispanic Black men compared with 3.0 ng/mL (95% CI = 2.8 to 3.2 ng/mL) for non-Hispanic White men. Overall, patient characteristics at diagnosis suggest that delayed detection contributed at least in part to increases in de novo metastatic disease.
近期研究表明,2010年至2019年期间,美国新发转移性前列腺癌的发病率有所上升。合理的解释包括在前列腺癌筛查建议后检测延迟,或与使用更敏感的成像技术相关的分期上调。利用监测、流行病学和最终结果患者病例,并对人口老龄化进行控制,我们发现在此期间,前列腺癌诊断时的中位年龄和前列腺特异性抗原(PSA)水平分别增加了1.4岁(95%置信区间=1.3至1.5岁)和1.4 ng/mL(95%置信区间=1.4至1.5 ng/mL),这与检测延迟假说一致。研究发现了种族差异,在此期间,非西班牙裔黑人男性诊断时PSA的第75百分位数增加了4.3 ng/mL(95%置信区间=3.7至4.8 ng/mL),而非西班牙裔白人男性为3.0 ng/mL(95%置信区间=2.8至3.2 ng/mL)。总体而言,诊断时的患者特征表明,检测延迟至少在一定程度上导致了新发转移性疾病的增加。