Department of Pediatric Surgery, Shengjing Hospital of China Medical University, Shenyang, China.
Ann Med. 2024 Dec;56(1):2417181. doi: 10.1080/07853890.2024.2417181. Epub 2024 Oct 23.
Bowel perforation is a major, yet unstudied complication of ultrasound-guided hydrostatic enema reduction (UGHR). In this study, we aimed to explore the risk factors and determine the clinical characteristics of bowel perforation during UGHR for paediatric intussusception (P-UGHR).
We retrospectively analysed the medical records of patients who underwent UGHR for intussusception at our institution between January 2011 and December 2021. The patients were divided into the P-UGHR and no P-UGHR groups. Univariate and multivariate logistic regression analyses were performed to analyse the risk factors for P-UGHR, and the clinical characteristics of patients with P-UGHR were determined.
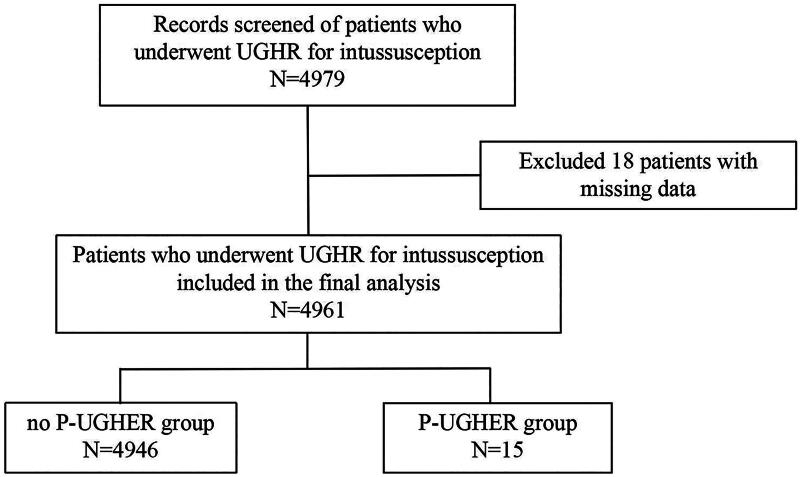
The final analysis included 4961 intussusception episodes. We identified 15 patients [eight male (53.3%); median age, 8.73 months; age range, 3-17 months] with P-UGHR. All P-UGHR cases involved colonic perforations without necrosis distal to the intussusception mass. The perforations were located in the ascending [40% (6/15)], transverse [46.7% (7/15)] or descending colon [13.3% (2/15)]. Age ≤10.5 months [odds ratio (OR), 3.636; 90% confidence interval (CI), 1.274-10.38; = 0.043], bloody stools (OR, 4.189; 90% CI, 1.352-12.978; = 0.037) and symptom duration >17.5 h (OR, 0.188; 90% CI, 0.053-0.666; = 0.03) were independent risk factors for P-UGHR.
Age ≤10.5 months, bloody stools and symptom duration >17.5 h were independent risk factors for P-UGHR. Caution should be exercised during UGHR in patients aged ≤10.5 months, with bloody stools or symptom duration >17.5 h.
肠穿孔是超声引导水压灌肠复位(UGHR)的一种主要但尚未研究的并发症。在本研究中,我们旨在探讨小儿肠套叠(P-UGHR)患者行 UGHR 时肠穿孔的危险因素,并确定其临床特征。
我们回顾性分析了 2011 年 1 月至 2021 年 12 月期间在我院行 UGHR 治疗肠套叠的患者的病历。患者分为 P-UGHR 组和非 P-UGHR 组。采用单因素和多因素 logistic 回归分析 P-UGHR 的危险因素,并确定 P-UGHR 患者的临床特征。
最终分析纳入了 4961 例肠套叠病例。我们发现 15 例患者(男 8 例,占 53.3%;中位年龄 8.73 个月;年龄范围 3-17 个月)发生 P-UGHR。所有 P-UGHR 病例均为结肠穿孔,且套叠肿块远端无坏死。穿孔部位位于升结肠[40%(6/15)]、横结肠[46.7%(7/15)]或降结肠[13.3%(2/15)]。年龄≤10.5 个月[比值比(OR)3.636;90%置信区间(CI)1.274-10.38;P=0.043]、血便(OR 4.189;90%CI 1.352-12.978;P=0.037)和症状持续时间>17.5 小时(OR 0.188;90%CI 0.053-0.666;P=0.03)是 P-UGHR 的独立危险因素。
年龄≤10.5 个月、血便和症状持续时间>17.5 小时是 P-UGHR 的独立危险因素。对于年龄≤10.5 个月、有血便或症状持续时间>17.5 小时的患者,行 UGHR 时应谨慎。